
記住我



Even though there have been major advances in biomedical research over the last decades, our survey of universities and hospitals in five European countries has shown that the collaboration between basic and clinical scientists is still far from being optimal in many organizations. Although successful collaboration is desirable, because it can speed up the success rate in the field, both basic and clinical researchers experience limitations in their daily work, which prevent them from efficiently interacting with each other. The research agenda in musculoskeletal diseases is still very long i.e. valuable treatment options in osteoarthritis and sarcopenia, personalised medicine, drugs that have durable bone-anabolic effects, and maybe even drugs that will favour a reestablishment of coupling between bone resorption and formation. To have success in this regard, we urgently need a stimulating translational collaboration in the field.
Our group, comprised of both basic and clinical scientists, has summarized the main barriers based on personal experience including (i) work overload (e.g. urgent clinical tasks), (ii) lack of common language and culture, (iii) infrastructure issues in the organizations (e.g. different buildings for basic and clinical research that are distant from each other) and (iv) lack of targeted funding of collaboration projects that play a critical role.
We also invited the opinion of managers/board members of our hospitals/universities, demonstrating a remarkable overlap in their responses. The interviewed managers collectively acknowledge the fact that collaboration between basic and clinical scientists is of paramount importance and will bring more scientific progress, and they all agree that regular collaborative scientific meetings and shared education programmes may be helpful. However, structural and/or financial support for translational collaboration between basic and clinical scientists is for most of them not (yet) on the top of their agenda.
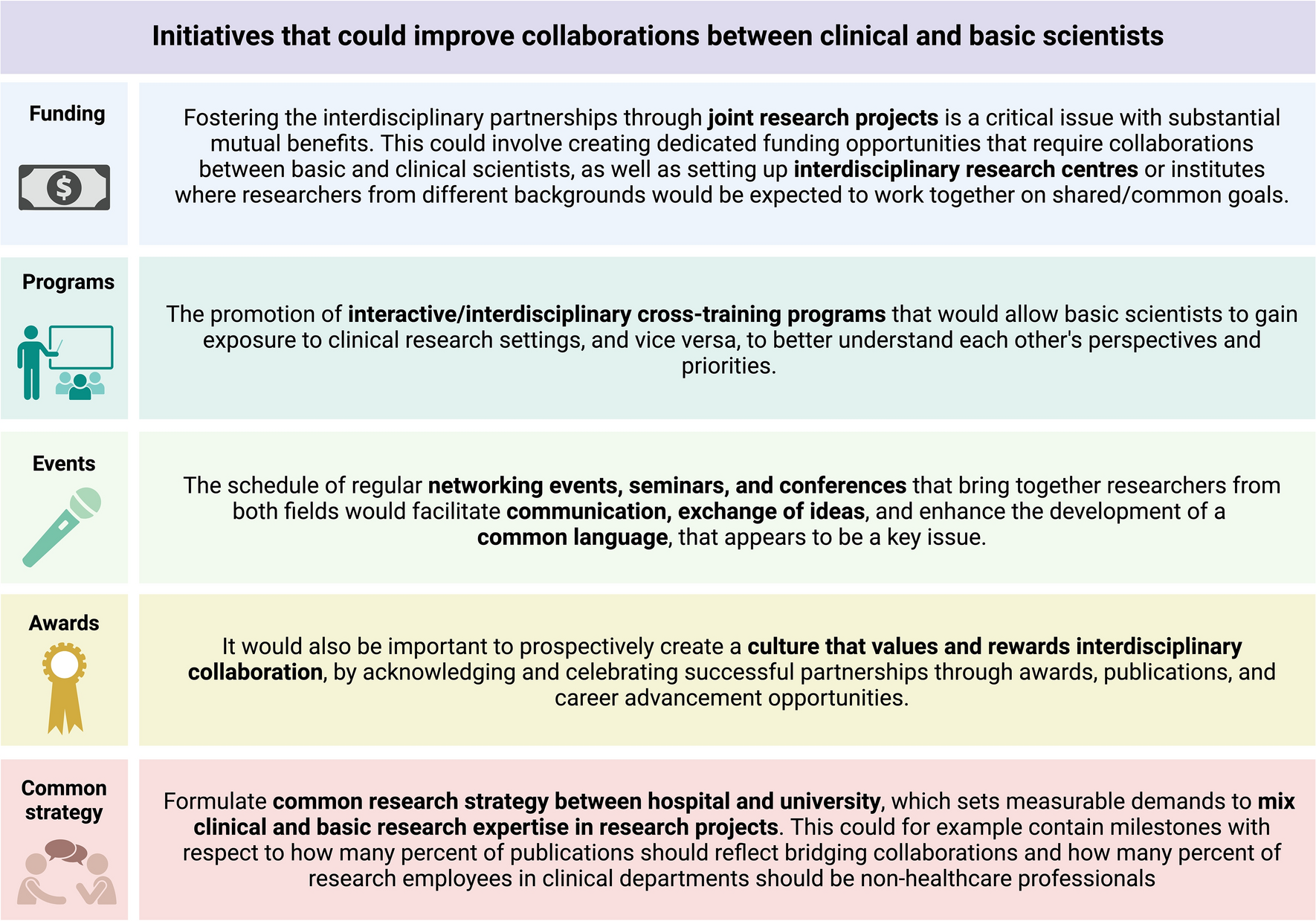
By analysing the collected responses and interviews of both basic and clinical scientists as well as managers, we have summarized below some suggested initiatives that would be perceived as effective from the scientists’ perspective (Fig. 1).
Fig. 1
Initiatives that could improve collaborations between clinical and basic scientists. Created with Biorender.com
Apart from the suggested initiatives presented in Fig. 1, the authors have also evaluated what is perceived as successful and effective existing initiatives at the home institutions of the authors. These examples are presented in a simplified manner in Fig. 2. One of these solutions to the translational problem in musculoskeletal diseases is to develop, promote, and expand the pool of clinician scientists, for example, through dedicated MD/PhD or clinician scientist programmes. This would be favourable to facilitate a more direct communication with basic scientists and thereby bring ideas from bench to bedside and vice versa. However, over the years, these experts have become rare, and with the enormous progress in both basic techniques, clinical opportunities, as well as work load they may be even more rare in the near future. Precisely therefore, creating more opportunities for basic and clinical scientists to work together will help to bridge the gap between these disciplines and foster a more integrated approach to biomedical research.
Fig. 2
Examples of successful initiatives as perceived by the authors. Created with Biorender.com
One may argue that our manuscript is too focussed on universities and hospitals. The situation seems to be different in pharmaceutical industries; based on a clear and strict hierarchy under one leader, all departments are working together on one theme, the development of a new drug such as the remarkably rapid and successful development of e.g. denosumab and romosozumab (as highlighted in the Introduction). This only highlights the strength of unifying, promoting, and coordinating the efforts of basic and clinical scientists. Although a similar coordinated and structured effort cannot be implemented one-to-one in the research efforts within academia and hospitals, it may be advisable to seek inspiration from the pharmaceutical industry when making efforts to optimise research efforts between academia and hospitals.
Finally, when scientific organisations such as ECTS, ASBMR (American Society of Bone and Mineral Research), and other national and international organisations plan meetings and conferences, it could be favourable to consider that participants may not always be limited to basic or clinical interests, but may actually be interested and engaged in both. When considering this, scientific conferences and meetings may be able to further stimulate coordinated research efforts between basic and clinical scientists.
In conclusion, this manuscript points out on the missing interactions between basic and clinical scientists and highlights the importance of fostering interdisciplinary collaboration between basic and clinical scientists in order to drive innovation and advances in musculoskeletal medicine. Today, more than ever, the scientific community recognizes that the future of biomedical research lies in the seamless integration of basic and clinical science, and that by working together, basic and clinical scientists can unlock new possibilities and make meaningful strides towards improving human health and well-being through personalised medicine and treatments that are more effective. We hope that our perspective will contribute to future discussions and activities to strengthen translational collaboration between basic and clinical science and to promote viable collaborative research strategies among hospitals, universities, and research institutions.
留言 (0)