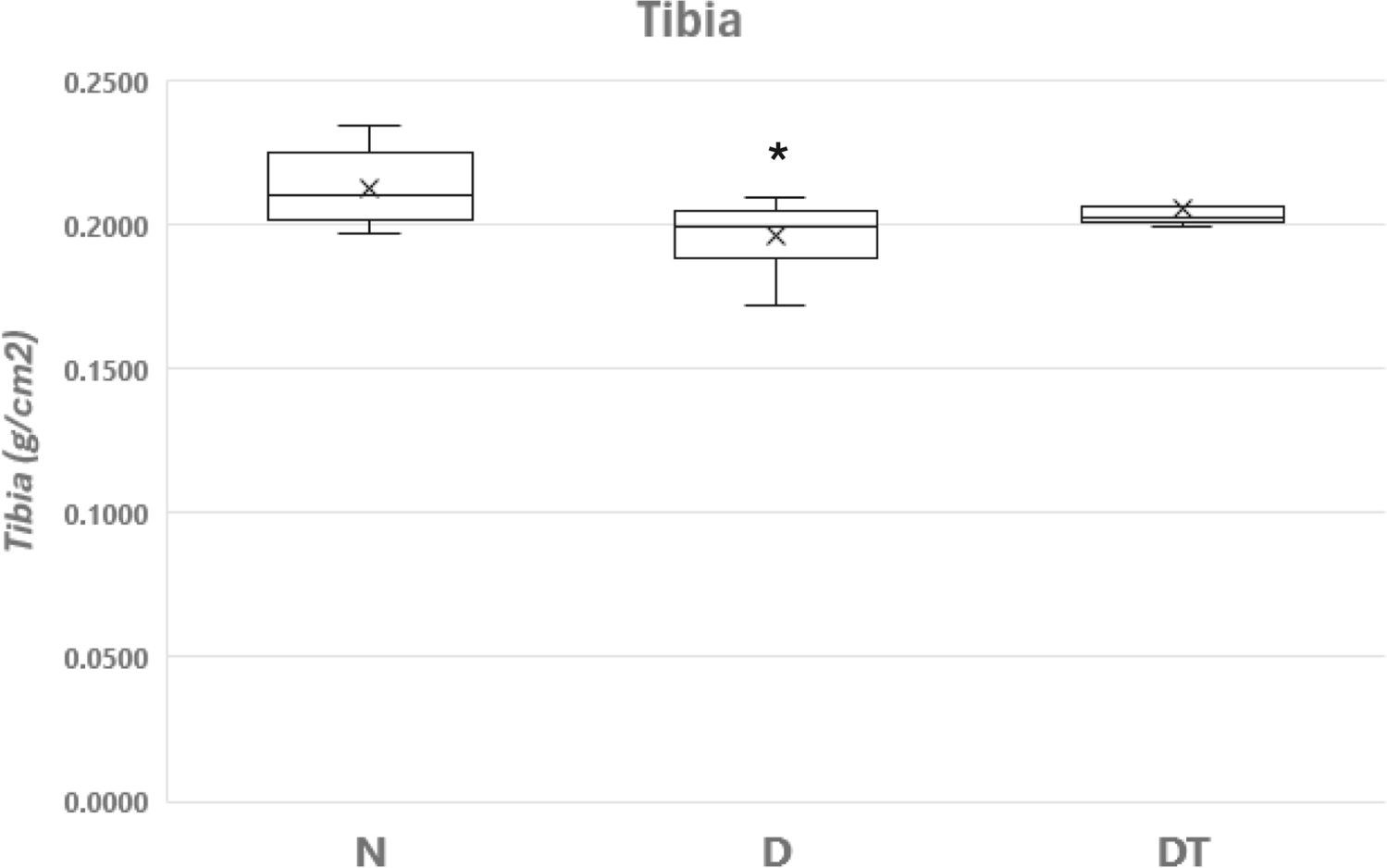
The 40% caloric restrictive diet was supplemented with additional vitamins and minerals where the only variable was the reduction in calories compared to the pair-matched normal fed sedentary group. The reduction in calories for the caloric restricted (D) group resulted in a 7.9% decline in bone mineral density and concomitant declines in bone mechanical properties of the tibia compared to the normal fed group (N). The decline in BMD in the current study is consistent with prior caloric restrictive studies in lean [23] and elderly female rats [24]. In contrast, BMD from the caloric restricted exercised group (DT) resulted in a 3.3% decline in BMD that was not significantly different compared to N. There were no significant BMD differences between DT and N or DT and D. Bone mechanical properties (Fmax and EF) were significantly higher for DT compared to D. While bone mechanical properties were lower for DT compared to N, they were not significantly different. Therefore, the results support our hypothesis that resistance training can mitigate bone loss and maintain bone health during severe caloric restriction.
Diets are typically employed to reverse obesity. However, emphasis on physical appearance and sexual appeal has been associated with being thin and become rampant in television ads, video games, and social media sites [3]. Collectively, the American population has become more self-conscious about body image resulting in the decision to engage in diets to lose weight even when it is not needed to reverse obesity [3]. This is especially apparent in normal weight young females who engage in diets due to body dissatisfaction, insecurity, and/or an inappropriate perception of what constitutes health/beauty [25]. In support, Latimer et al. [26] reported that 28% of American college students were trying to lose weight even though they were under- or at a normal body weight. Wharton et al. [27] reported over 73% of young American women attempted to lose weight even though 78% were normal or underweight. In addition to the media exposure emphasizing thinness, there is scientific interest in understanding the impact of caloric restrictive diets in humans given the reports that diets can extend the lifespan in animals [28]. In particular, the primary purpose of the CALERIE (Comprehensive Assessment of Long-term Effects of Reducing Intake of Energy) trials, supported by the National Institute on Aging, is to determine parallels and/or disparities in humans compared to previous findings in animals. Collectively, the media exposure that emphasizes being thin and the association between caloric restriction and lifespan may prompt a myriad of non-obese individuals to engage in diets [29]. However, the impact of caloric restrictive diets in normal weight individuals has the potential to negatively impact bone health. In support, a report from the CALERIE trials in healthy, non-obese men and women indicated bone loss at osteoporotic fracture sites when they engaged in ~ 25% caloric restrictive diets [5]. In like manner, we observed lower bone mineral densities in the femur from non-obese women who reportedly consumed 55% of their recommended minimum daily requirement [30]. Further, a systematic review of major databases done by Veronese and Reginster [31] revealed a significant reduction in BMD associated with caloric restrictive diets thereby compromising bone health.
A decline in bone health is a natural process of aging where the prevailing bone disease associated with senescence is osteoporosis. Data from the U.S. Census Bureau suggest that the elderly are the fastest growing population in the United States [32]. In the past decade, the 65- and older population grew by 34.2% [32]. Considering the elderly population trends, osteoporosis has the potential to approach epidemic levels [33] where the prevalence of this disease has been known to impact more women than men [34]. Moreover, if caloric restrictive diets are implemented by normal weight young women to obtain a thin body image, the projections for osteoporosis may exceed what is anticipated due to senescence alone. Given the absence of a cure for osteoporosis, prevention becomes of utmost importance where resistance training is an effective method to stimulate an elevation in bone mass that will delay the onset or reduce the severity of bone fractures later in life.
There are numerous reports regarding the use of exercise in the overweight and obese population to attenuate the loss of bone during caloric restrictive diets [1, 2, 35]. However, human studies specifically examining the impact of exercise to prevent or mitigate bone loss associated with caloric restrictive diets in normal weight individuals are uncommon. This is most likely due to the challenge in human data collection and/or prior animal studies that have shed light on the outcome minimizing the need to engage in numerous human studies. In support, Bloomfield’s lab reported that during a 40% energy restrictive diet, treadmill running 3–4 times per week offered a partial protection from tibial bone loss in female rats [10,11,12]. In another well-controlled study employing treadmill exercise during moderate caloric restriction (20% overall less energy) and severe caloric restriction (40% overall less energy) [13], they reported few adverse effects on the femur with the moderate caloric restriction combined with exercise. Meanwhile, the combined impact of exercise during severe caloric restriction mitigated the detrimental effects on bone compared to caloric restriction in the absence of exercise [13]. In this study, bone mechanical properties were assessed where severe energy restricted exercised female rats demonstrated a trend toward greater structural properties of the femur compared to severe energy restricted controls [13]. The results of the current study support all their treadmill findings [10,11,12,13] and demonstrate that resistance training can also attenuate bone loss in the tibia associated with a 40% caloric restrictive diet, but we also note some differences. The treadmill running studies employed a 12-week caloric restrictive diet and noted improved structural tibial bone properties [10,11,12] and elevated bone mechanical properties of the femur [13]. In contrast, we administered a 40% caloric restrictive diet for 6 weeks where our resistance training protocol resulted in improvements in tibia BMD and significant elevations in bone mechanical properties (i.e., Fmax and EF) for the DT group compared to the pair-matched D group. Therefore, the more rapid training-induced alterations in BMD support the enhanced effectiveness of strength exercise during caloric restriction. Further, the enhanced tibial bone mechanical properties for DT vs. D confirm the improved structural bone properties noted by prior exercise studies [11, 12, 36] and the elevations in bone mechanical properties observed in the femur [13]. In opposition to the current results and prior treadmill studies in rats, McGrath et al. [37] implemented a 30% caloric restrictive diet in female mice and reported that 6 weeks of chronic exercise had a negative impact on the femur. They implemented voluntary wheel running where the caloric restricted animals averaged 10 km/day [37]. In contrast, the forced treadmill running employed by others [10,11,12,13] required rats to run 3–4 days/week and the distance covered per exercise session was 4 to 8 times lower than the mice reported by McGrath et al. [37]. Thus, it is possible that more prolonged and/or daily aerobic exercise during caloric restriction, as observed by McGrath et al. [37], can eventually yield detrimental effects on the bone. Next, Hattori et al. [38] examined the impact of voluntary wheel running combined with a 30% caloric restrictive diet in adult male rats and found no changes in bone loss, bone morphology or bone strength of the tibia compared to sedentary controls [38]. We have no explanation for the discrepancy among the various caloric restrictive diet studies in animals. However, we recognize the potential for sex differences and/or the use of prolonged daily running as the mode of exercise compared to treadmill exercise or resistance training three times per week.
Despite the disparities from prior animal studies pertaining to running as the mode of exercise, the strength training-induced maintenance of BMD for DT compared to N is consistent with our prior reports on the effectiveness of this mode of exercise in promoting an osteogenic response in maturating animals [15,16,17,18,19,20]. Further, the current report confirms previous findings in humans [39,40,41] and animals [15,16,17,18,19,20, 42, 43] pertaining to higher osteoblast activity as the potential mechanism for the reported maintenance of BMD as supported by the serum OC from the DT and N groups. Accordingly, the lower serum OC for D vs. N also supports the potential mechanism for the reductions in BMD attributable to caloric restriction, i.e., a reduction in osteoblast activity. Last, our results regarding training-induced elevations in bone mechanical properties of the tibia are also consistent with our prior reports [15,16,17,18,19] and others that have examined the femur after treadmill running [13], jumping exercise [36], and tower climbing [44] in normal fed rats vs. sedentary controls. Therefore, the elevation in bone mechanical properties for DT is consistent with the higher BMD compared to D. Collectively, the current results emphasize the importance of incorporating resistance training to maintain bone health during severe caloric restriction.
Finally, we recognize several limitations of this study. First, given the impact of hormones upon the bone, it would have been prudent to measure insulin-like growth factor, estrogen, parathyroid hormone, and/or leptin. Next, assessing BMD and serum markers for all animals prior to the implementation of the study would have allowed for a longitudinal assessment. As it pertains to BMD, the DXA measures mass per area where differences in bone size can result in misinterpretations with the use of DXA [45]. In addition, DXA does not provide information regarding bone microarchitecture. As such, we acknowledge that having access to micro-CT (micro-computed tomography) or pQCT (peripheral quantitative computed tomography) as well as histomorphometry data and/or employing tartrate-resistant acid phosphatase to assess osteoclast number would have added to our interpretation of the results. We also recognize that bones were stored in an ethanol/saline solution at room temperature where potential changes in the organic matrix due to the ethanol as well as potential denaturation of proteins were possible that could alter the mechanical testing results. However, the tibia was treated in the same manner for all groups prior to bone testing that allows for relative comparisons. Despite all these limitations, the bone mechanical properties supported the alterations in bone mineral density for a given group. Further we acknowledge the small sample size for each group that may have prevented achieving statistically significant differences between groups for several measurements. Given the limited amount that is awarded for internal grants, we were confined to focus on the major factors after the experimentation that would either support or refute our hypothesis. Last, our study employed 6 weeks of caloric restriction. Thus, it is possible that strength training during more prolonged caloric restriction may yield different results.




留言 (0)