This study highlights the intricate relationship between sexual function, androgen levels, and body image perception among women with TS, recognizing the impact of significant phenotypic differences associated with distinct karyotype. These results underscore the potential contribution of hormonal imbalances to body image dissatisfaction and sexual dysfunction in patients with TS.
To fulfil this purpose, participants were classified into four groups based on karyotype distinctions, as similarly performed in a Chinese study conducted in 2019 [33].
Frequency of spontaneous menarche varied according with karyotype: all 45, X monosomy required puberty induction, whereas those with some 46, XX cell lines mostly experienced spontaneous menarche. Individuals with mosaic patterns or structural alterations of X chromosome were less likely to require puberty induction than those with mosaic patterns [4]. Consistent with these results, Cameron-Pimblett and colleagues reported a lower primary amenorrhea prevalence in patients with X isochromosome and X ring chromosome compared to those with 45, X karyotypes [4].
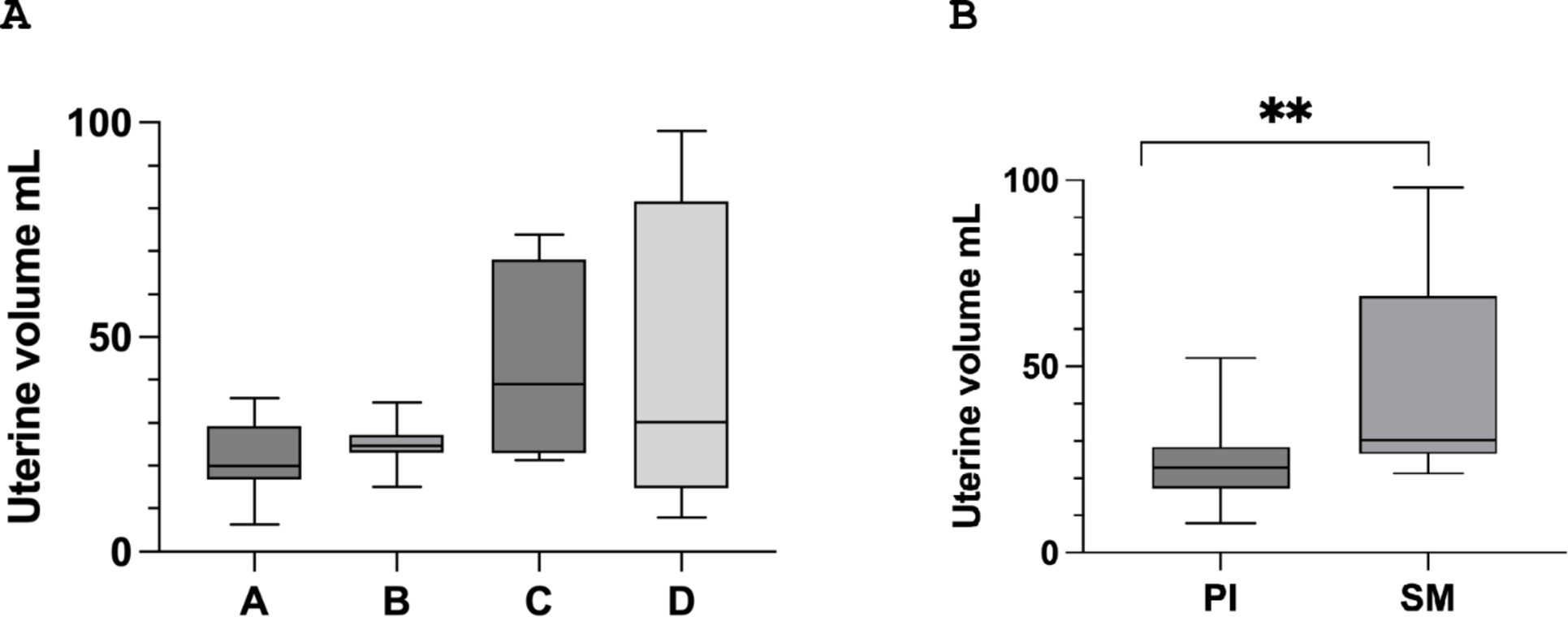
In another study, patients were categorised according to the karyotypes into groups 45, X, 45, X/46, XX, corresponding to our groups A and D respectively, and a “miscellaneous” group equivalent to our groups B and C. This study showed a decreasing trend in the onset of ovarian insufficiency from the monosomy group to the mixed group, and further to the group with some 46, XX cell lines [10]. We further demonstrated a greater uterine volume in women with spontaneous menarche compared to those requiring puberty induction, emphasizing the importance of achieving sufficient uterine growth, especially for fertility considerations [1]. However, uterine volume did not reach normal levels in patients undergoing puberty induction and remained below the average size reported in nulliparous, non-hypogonadal women [34].
The feasibility of achieving normalisation of uterine volume varies across studies, with some reporting it as achievable with tailored pubertal induction protocols, whereas others report persistent limitations [35,36,37]. However, this effect was not observed in this cohort, possibly due to incomplete dosing details and variability in pubertal induction protocols, which limit definitive conclusions. Lastly, no karyotype-based differences in uterine dimensions were found, in agreement with prior research [37].
Hormonal analyses revealed lower levels of cfT, FAI and DHEA-S in Group A compared to group D. These findings are consistent with the known effects of “streak gonads,” where reduced ovarian function leads to minimal androgen production, particularly ∆4 and TT [38]. Notably, within the group that experienced spontaneous menarche, TT, cfT, FAI, and DHEA-S levels were significantly higher. This supports the notion that spontaneous ovarian activity correlates with increased androgen production. However, the reduced levels of DHEA-S, primarily secreted by the adrenal glands, suggest that adrenal androgen production could also be compromised in patients with TS. This phenomenon appears particularly evident in patients with a pure 45,X karyotype, often associated with a more severe clinical phenotype. The greater severity of ovarian dysgenesis in these patients might inherently affect adrenal function, potentially through shared developmental or hormonal pathways. Lower adrenal androgen levels in these patients could also reflect systemic factors, such as metabolic stress, elevated insulin levels, chronic inflammation, or coronary pathologies, all of which have been linked to reduced DHEA-S production in other populations [39,40,41]. Consequently, patients with more severe karyotypes may exhibit a broader disruption of androgen levels extending beyond the ovaries. These results are consistent with those reported in the recent study conducted by Viuff et al., the most extensive research investigating serum levels of sexual hormones in patients with TS [18]. However, the Danish study included only three patients receiving TD therapy and no subdivision based on karyotype was performed. Some research suggests that exogenous oestrogens in HRT might reduce DHEA-S levels, but the exact mechanism remains unclear [42, 43]. These observations underscore the multifactorial nature of hormonal imbalances in TS, highlighting the need for further studies to elucidate the underlying mechanisms driving androgen reductions and their interaction with karyotype, adrenal function, and systemic factors.
It is well known that oral HRT induces an increase in SHBG, leading to a further decrease in bioavailable androgens [44]. The higher levels of SHBG observed in the oral therapy group confirm existing data in literature and highlight a greater hepatic effect of oral oestrogens than TD formulation [45]. Surprisingly, in contrast to existing literature, reduction of LH levels was greater in TD vs. oral route [46]. This, in our opinion, could be attributable to the poor compliance, especially in the early stages of TD HRT, that may be observed among patients.
To date, this research is one of the few studies that assess sexual function in patients with TS, firstly indicating that about 50% of patients are sexually active, in line with the previous literature [25, 47]. Our findings diverge from other studies on the presence of FSD in sexually active patients [25,26,27, 47, 48]. For instance, in a study conducted by Ros and colleagues, sexually active patients with TS showed scores comparable to both a control population and patients with hypogonadotropic hypogonadism, except for the arousal domain; however, this study did not provide scores for individual domains or the percentage of patients with a pathological response to the FSFI questionnaire [25]. In the investigation carried out by van den Hoven et al., it was reported that 80% of patients with TS expressed satisfaction with their sexual life, although specific data were not provided. Although four different questionnaires related to sexual function, including FSFI, were administered, none of the results were reported, and the definition of satisfaction remained unspecified [47]. Contrasting with previous literature, suggesting a satisfactory sexual life in patients with TS, our study indicates a high prevalence of FSD, potentially linked to relational and physical challenges. This information emerged not only through the survey responses but was also communicated by the patients themselves during their visits. We believe this may be due to the importance attached to this topic during our medical consultations and an appropriate care setting. In this cohort, seven women, five of whom were sexually active, practised autoeroticism. A previous study that explored the likelihood of masturbation in these patients reported lower rates than in healthy controls or individuals with other disorders of sexual development, but comparable to those observed in individuals with partially virilising XY disorders [49]. However, the percentage identified in another study was higher compared to that emerged from our study, yet it remained lower than the general population [27]. About this issue, a recent Spanish study included an interview conducted among patients with TS, revealing the perception that healthcare professionals were not interested in their sexual activity, relationship with their body, and masturbation, “experienced their sexuality under a cloak of silence” [50].
No differences in FSFI scores were observed between patients practising autoeroticism and others. This could be clarified by other unexamined factors; for example, in a recent survey, women who practised autoeroticism more frequently were also less satisfied with sexual activity with their partner [51]. Conversely in other studies, women practising autoeroticism were found to be more sexually active and more satisfied with sexual activity [52].
Among the participants, higher SHBG levels were associated with improved pain scores and less frequent pathological FSFI responses. These findings suggest that SHBG may serve as a marker of oestrogenic activity and underline the significant role of oestrogens in influencing specific domains of sexual function, particularly pain modulation [53]. However, androgen levels did not show significant correlations with overall FSFI scores.
We found no differences in body image perception outcomes across various chromosomal anomalies, and about 45% of the study sample exhibited a potential disorder in body image perception [29]. This corresponds with observations from the limited available literature, including a 2020 study reporting a comparable prevalence of 37% among patients with TS [27, 28]. The results related to karyotype are partly conflicting compared to those obtained from a similar study conducted on adolescent girls with TS; however, the latter study employing a different questionnaire, the “Multidimensional Body-Self Relations Questionnaire”, demonstrated that patients with a pure karyotype had a poorer perception of body image compared to those with mosaic karyotype. Nevertheless, this observation was not confirmed in the multiple linear regression analysis including age, race, and socio-economic status [28].
Avoidance behaviours, as measured by the BUT-A, were correlated with pathological FSFI scores, highlighting the associations between body image discomfort and sexual distress. This is consistent with evidence from non-TS cohorts, where body image dissatisfaction has been shown to significantly impact sexual well-being [54]. Additionally, lower testosterone levels in this population were inversely correlated with higher pathological BUT-A scores, suggesting that testosterone may play a critical role in modulating body image perception [54]. These results align with a pilot study conducted by Zuckerman-Levin et al., which demonstrated that androgen replacement therapy in women with TS improved aspects of cognitive function, quality of life (QoL), and sexual desire [55]. Collectively, the data suggest that oestrogens, mediated by SHBG, predominantly influence physical aspects like pain, whereas androgens may be more critical for psychological and relational dimensions of sexual health. The interplay between oestrogens and androgens in female sexual health is multifaceted. Oestrogens primarily influence lubrication and pain modulation through central and peripheral mechanisms and androgens are more directly involved in sexual desire and arousal, acting via the dopaminergic reward system [53, 56]. In this cohort, elevated SHBG levels likely reflect increased oestrogenic activity, contributing to improved pain scores. However, the observed reduction in bioavailable androgens could limit benefits related to sexual desire and body image perception. This highlights the distinct yet complementary roles of these hormones, underscoring the need for further studies to explore optimal hormonal strategies in TS patients.
Finally, the role of height in body image was also explored, revealing a non-significant trend suggesting that shorter stature might contribute to a more pathological perception of height. This observation is consistent with studies highlighting the psychological challenges associated with short stature in TS [57, 58]. However, adult height has not been found to significantly influence overall QoL in TS [58]. Moreover, recent evidence suggests that body image challenges in TS are multifactorial, involving not only physical traits like height but also broader psychosocial and relational factors [28].
This study has several limitations that should be acknowledged. The main limitation is represented by the small sample size, although it is crucial to acknowledge that TS is a rare disease. Another major limitation of this study is that androgen levels were not measured using mass spectrometry. Additionally, the duration of HRT was not uniform, and this may have partially influenced the results. Nevertheless, the minimum therapy duration at the time of evaluation was one year. Moreover, the lack of assessment of sexual-related distress represents another limitation of this study. Although tools such as the Female Sexual Distress Scale are available for evaluating this parameter, no officially validated Italian version currently exists, which influenced our decision not to include it. An additional limitation is that, although orgasmic function was evaluated in this study using the FSFI, we acknowledge the absence of a psychometric tool specifically validated to measure orgasmic intensity, such as the Orgasmometer-F [59]. Finally, we encountered challenges in obtaining detailed information about pubertal development, dosing and time used for pubertal induction and our assessment was limited to relying exclusively on the occurrence or absence of spontaneous menarche.




留言 (0)