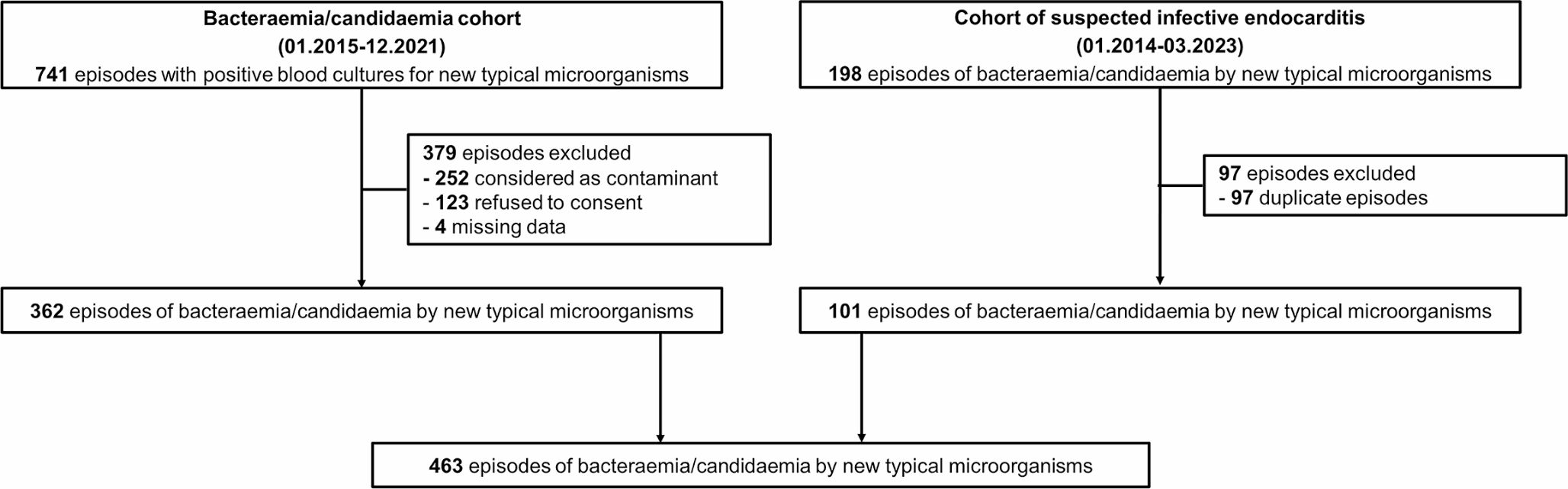
This retrospective study was conducted at Lausanne University Hospital in Switzerland from January 2014 to March 2023. The study integrated data from two separate cohorts: bacteraemia/candidaemia cohort (January 2015 to December 2021), and non-duplicate episodes from the cohort of patients with suspected IE (January 2014 to June 2023; suspicion of IE was defined as blood cultures drawn and echocardiography performed specifically for the research of IE).
Included microorganisms were divided in two Groups. Group A comprised of microorganisms that were considered typical regardless of the presence of intracardiac material (S. lugdunensis, Granulicatella spp., Abiotrophia spp., Gemella spp.), and Group B consisted of those that we considered typical only in the presence of intracardiac material (CoNS other than S. lugdunensis, C. acnes, C. striatum, C. jeikeium, P. aeruginosa, S. marcescens, non-tuberculous mycobacteria, and Candida spp.).
Inclusion criteria encompassed adult patients (≥ 18 years old) with at least one positive blood culture for.
any Group A microorganism, or.
any Group B microorganism along with either presence of intracardiac prosthetic material or cardiac imaging studies performed.
Exclusion criteria included patients who had formally declined the use of their data, cases with incomplete medical records (including patients transferred to other hospitals at the onset of infection without follow-up data), and instances where isolated microorganisms were considered contaminants (if only one positive blood culture set grew a skin contaminant).
Data on demographics (age, sex), demographic, clinical, imaging, microbiological, surgical, and pathological were retrieved from patient’s electronic health charts.
Blood cultures bottles (aerobic: BD Bactec Plus aerobic/F; anaerobic: BD Bactec Lytic/10 anaerobic/F) were drawn and incubated in a BACTEC FX 400® (BD, Becton Dickinson, Franklin Lakes, NJ, US) for 14 days when endocarditis or candidaemia were suspected (if not labeled, the blood cultures were incubated for 5 days). Species identification in the species level was performed directly from blood culture pellets as well as from subcultures using matrix-assisted laser desorption-ionization time of flight mass spectrometry (Bruker Daltonics Inc., Billerica, MA, USA). From 2014 to 2018, blood culture pellets were obtained using the method described by Croxatto et al. and since 2019, the rapidBAC PROTM II (Nittobo, Tokyo, Japon) was used [21, 22]. When MALDI-TOF score was inconclusive (< 1.8 for blood culture pellets or < 2 for subculture colonies), a protein extraction was performed before analysing the spectra MALDI-TOF again. Briefly, 25 µl of blood culture pellet or ~ 1 µl of colonies were resuspended in 500 µl of sterile water at 13,000 g for 2 min at room temperature. After discarding the supernatant, the pellet was resuspended with 70% formic acid, followed by the addition of 100% acetonitrile and vortexing for one minute. After another centrifugation under the same conditions, the sample was prepared for analysis by drying two deposits on a target plate at 35 °C and adding 1 µl of matrix before the final drying step.
When there was a suspicion of mycobacterial infection, lithium heparinate samples were drawn from patients and subsequently incubated in BD Bactec Myco/F-Lytic culture vials for 42 days (BD, Becton Dickinson, Franklin Lakes, NJ, US). Mycobacteria species identification was then performed using a 16 S rRNA PCR and Sanger sequencing as previously described [23].
In our institution, notifications regarding patients with positive blood cultures were received by infectious diseases (ID) consultants, but the decision to conduct an ID consultation was left to their discretion. However, for all patients with candidaemia or those with suspected IE, an ID consultation was mandatory. In January 2018, an Endocarditis Team was established, and since then, the diagnosis of IE has been determined by the Endocarditis Team. For all cases prior to 2018, the IE diagnosis (reference standard) was made by two IE experts (MPO and PM) in an a posteriori and consensus approach, after reviewing clinical, laboratory, microbiological, imaging, surgical, and histopathological findings from patients’ medical records, and not on the classification of the Duke criteria. To ensure consistency and continuity in diagnosis, both expert clinicians were members of the Endocarditis Team. Cases were further categorized as rejected, possible, or definite IE according to the three versions of the Duke clinical criteria (2015 Duke-ESC [1], 2023 Duke-ESC [13], and 2023 Duke-ISCVID [4]).
The date of collection of the first positive blood culture was defined as the onset of infection. A new episode was included if more than 60 days had passed from the first negative blood culture for the initial bacteraemia/candidaemia. True bacteremia was defined as the identification of a common skin contaminant isolated from at least two separate blood culture sets, combined with the decision by the patient’s physician to treat the identified pathogen. The determination of the infection site was based on the assessment by the ID consultant, taking into account clinical, radiological, microbiological, and operative findings.
SPSS version 26.0 (SPSS, Chicago, IL, USA) was used for data analyses. Categorical variables were analyzed using the chi-square or Fisher exact test and continuous variables with Mann–Whitney U test. The efficacy of each version of the Duke clinical criteria was evaluated by measuring the level of agreement between the reference standard and either definite IE cases or definite/possible IE cases. Sensitivity, specificity, positive and negative predictive values (PPV, NPV) and accuracy were calculated with a 95% confidence interval (CI). All tests were 2-tailed, and a significance level of P < 0.05 was applied.

留言 (0)