Design and study population
This retrospective observational study was conducted in Switzerland over a period of 13 years (2010–2022). Cases of P. aeruginosa BSIs were included from laboratories of 78 Swiss acute care hospitals that reported data to the Swiss Center for Antimicrobial Resistance (ANRESIS) in 2010 and 2022 and for more than half of the years within this period. All five university hospitals in Switzerland were reporting data to ANRESIS and were included in the study.
Data collection and processing
The P. aeruginosa BSI data were obtained from the ANRESIS database [25]. The participating laboratories are distributed all over Switzerland and accredited by national authorities. Deduplication was performed by counting only one isolate per patient and year– more precisely, in each case, the most resistant isolate.
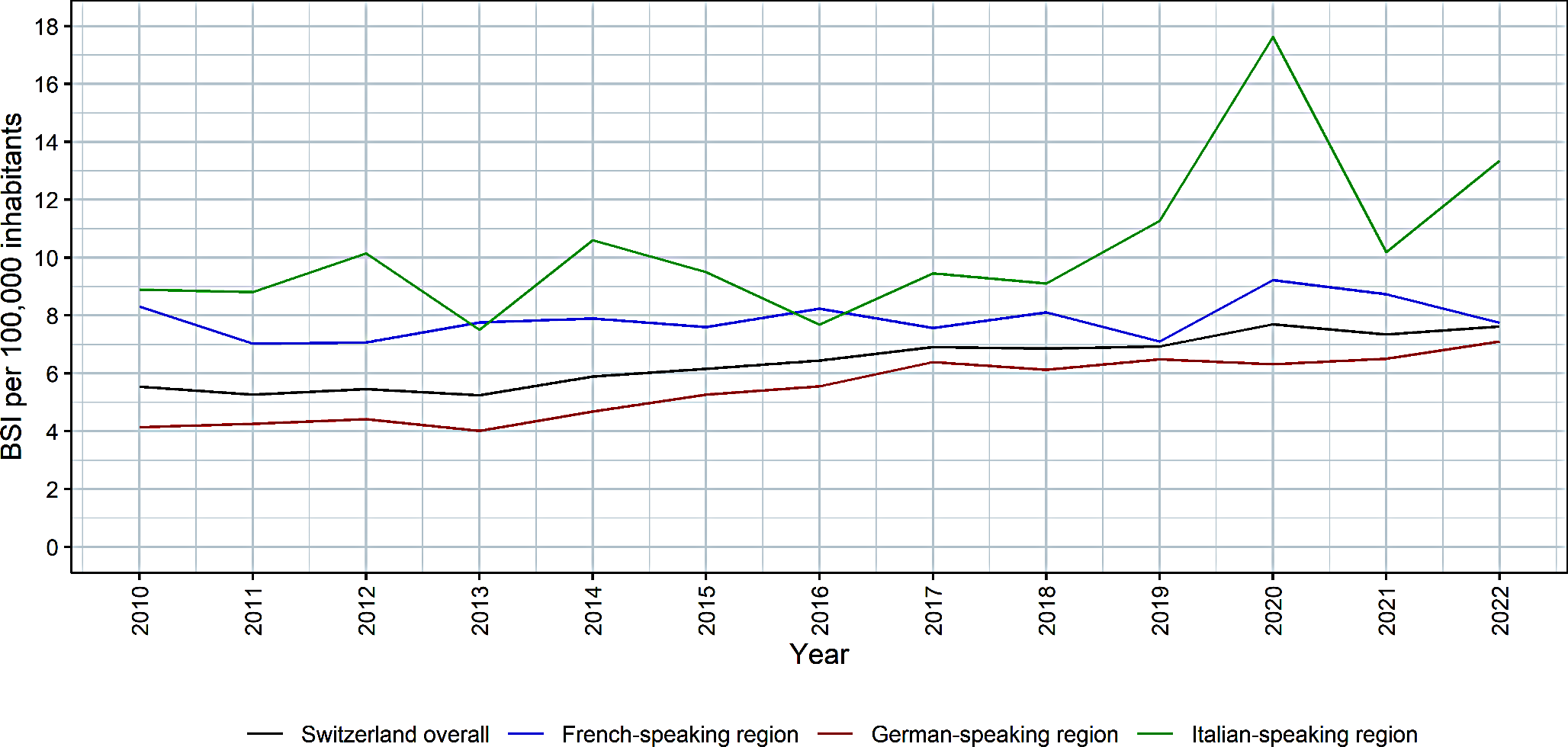
First, the overall incidence of P. aeruginosa BSIs per 100,000 inhabitants in Switzerland was analyzed by extrapolating the number of cases per 100,000 inhabitants by the coverage of the included hospitals, assuming that all patients with P. aeruginosa BSIs are hospitalized. In 2010, the overall coverage in Switzerland was 59.0%, in 2022 59.3% and in 2017, the median year in the study period, the coverage was 58.1%. The calculation was based on the yearly bed-days of the 78 included acute care hospitals covered by ANRESIS. With the abovementioned inclusion criteria for hospitals, regularly delivering data within the study period, the variability of reporting hospitals was low, and therefore, the coverage in the median year was used throughout the whole study period.
Second, the incidence in the three main linguistic regions was calculated. In 2017, the coverage of yearly bed-days in the French-speaking region was 74.2%, the coverage in the German-speaking region was 52.1% and the coverage in the Italian-speaking region was 71.3%.
Third, the resistance rates and incidences of six antibiotics/antibiotic categories and MDR strains, including aminoglycosides, carbapenems, ceftazidime, cefepime, ciprofloxacin, and piperacillin-tazobactam were analyzed. Resistance was defined according to the ANRESIS-restricted definition [26]. In detail, for aminoglycosides, the entire category was considered resistant if P. aeruginosa was resistant to amikacin and/or gentamicin. The carbapenem category was considered resistant if P. aeruginosa was resistant to imipenem and/or meropenem. MDR was defined as resistance to three or more of five antibiotics/antibiotic categories [26]. For this definition, ceftazidime and cefepime were combined into one category.
Descriptive subgroup analyses were performed to assess the incidence and resistance rates in different age groups (< 2 years, 2–24 years, 25–49 years, 50–64 years, 65–79 years, and ≥ 80 years) and for males and females.
The yearly number of inhabitants in Switzerland and in each linguistic region was used as the denominator and was adjusted for sex and age group in the corresponding analyses [27]. In addition, a pooled resistance rate over the whole study period was calculated for each age group.
During the study period, the guidelines for antibiotic susceptibility testing and breakpoints changed from the Clinical & Laboratory Standards Institute (CLSI) to the European Committee on Microbial Susceptibility Testing (EUCAST), which is used by all but one laboratory. However, breakpoints for the definition of resistant P. aeruginosa did not change or changed only marginally and should not have affected the results [28].
In an additional post hoc analysis, the percentage of P. aeruginosa BSIs among all BSIs was calculated for each year of the study period. If P. aeruginosa was detected in at least one blood culture, the patient was considered to have a BSI with P. aeruginosa.
Statistical analysis
First, temporal trends in the incidence of P. aeruginosa BSIs per 100,000 inhabitants were analyzed for Switzerland overall by fitting separate Poisson regression models for overall incidence and resistant isolates against aminoglycosides, carbapenems, cefepime, ceftazidime, ciprofloxacin, piperacillin-tazobactam and MDR P. aeruginosa. In a second step, possible trends in the different Swiss linguistic regions were considered by fitting Poisson regression models including the predictor variables year, linguistic region and the interaction between year and linguistic region.
Furthermore, logistic regression models were used to analyze the trends in the percentage of isolates resistant to aminoglycosides, carbapenems, cefepime, ceftazidime, ciprofloxacin, piperacillin-tazobactam and MDR P. aeruginosa among all P. aeruginosa BSIs in Switzerland. In addition, possible trends in resistance rates in the different Swiss linguistic regions were considered by applying multiple logistic regression models, including the predictor variables year, linguistic region and the interaction between year and linguistic region.
The results were considered significant if the p values of the likelihood ratio test and the t test of the explanatory variable were less than 0.05. Due to the small sample size in the Italian-speaking region, the results from the trend analyses including the Italian-speaking region are reported in the supplementary information only, to avoid misleading information. All analyses were performed using R software (version 4.2.2., R Core Team, Vienna, Austria).

留言 (0)