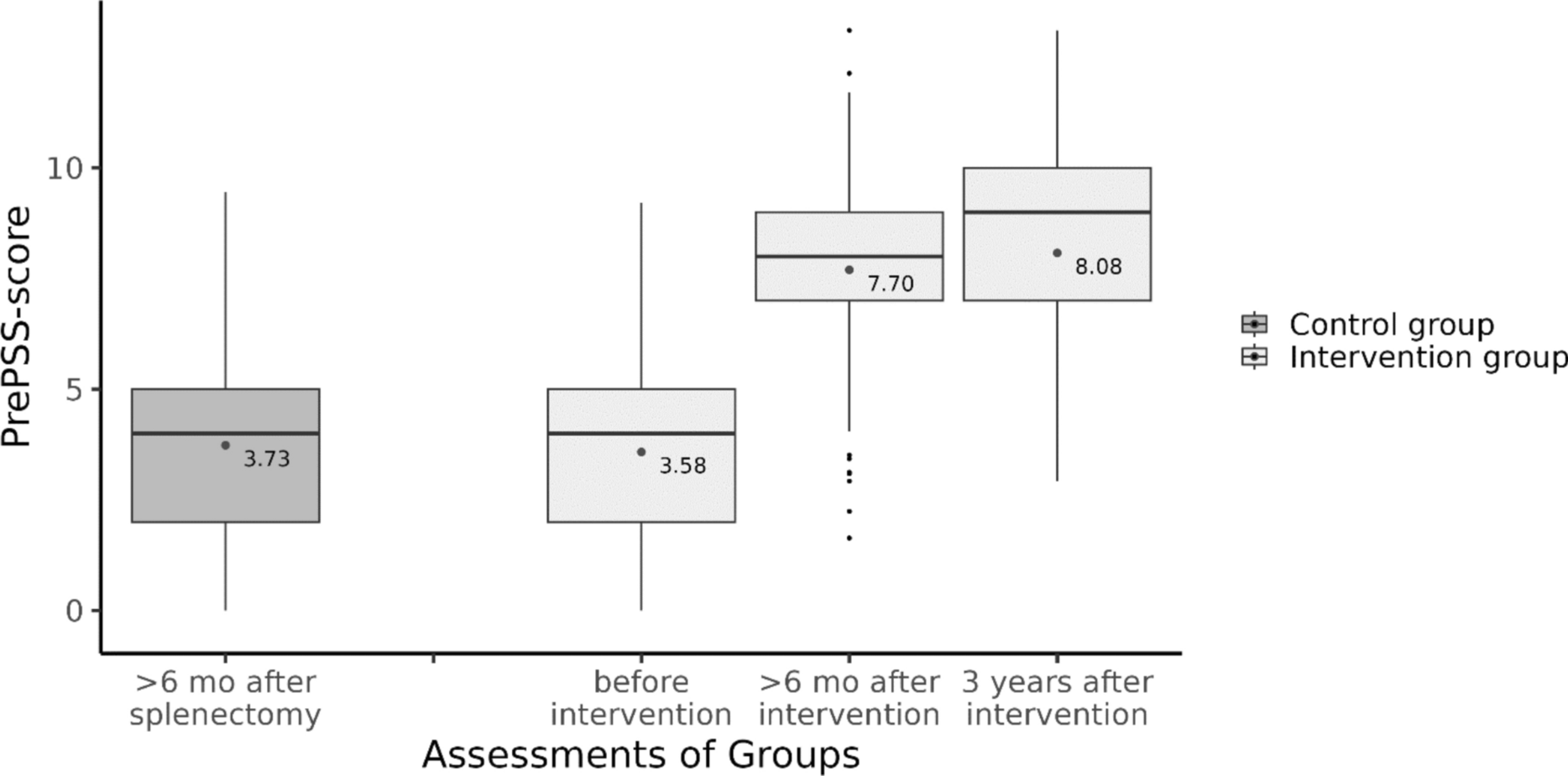
Following up on our prospective controlled cohort, we were able to demonstrate that a novel telephonic HAPA-based intervention led to sustained improvements in adherence to recommended preventive measures in asplenic patients. Three years after the intervention overall PrePPS scores increased as did individual vaccination coverage.
We observed a comparatively high follow-up completion rate, with 79 out of 88 surviving patients (90%) successfully followed up after three years. The relevant number of deaths (18/106, 17%) is partly to be expected because splenectomy is increasingly performed for non-traumatic reasons with the main reason being a malignant disease [16], [10]. In our cohort, the percentage of patients suffering from malignoma was even higher than in the literature with more than half of the patients undergoing splenectomy for hematooncological reasons. Prognosis in such a cohort is limited compared to studies analyzing patients after traumatic asplenia [14]. Additionally, it is highly likely that our data underestimate underlying disease as cause of death since multiple patients who failed to respond to our efforts or who were confirmed to be dead by next of kin were known to suffer from advanced malignoma since before the inclusion in the study.
The long-term effects of telephonic interventions are subject to ongoing debate and seem to depend heavily on the actual intervention. A review by Tonapa and colleagues found, e.g., that telecoaching in patients with heart failure improved self-care behaviour and quality of life. However, follow-up times were quite short (range 3–9 months) and longterm effects thus not studied [15]. On the other hand two RCTs studying the effect of a digital intervention on depressive symptoms in diabetic patients found that albeit there was a significant improvement three months after the interventions, these effects had vanished after six months of follow-up [2]. Following our intervention, however, according to the PrePSS score preventive measures were upheld for or even re-newed after three years (e.g. seeking recommended re-vaccinations, renewing antibiotics prescriptions). The robustness of this effect may in part be due to the high degree of patient involvement and empowerment using a HAPA based methodology. The efficacy of this intervention is possibly even greater because of the nature of most of the recommended preventive actions. Vaccinations, e.g., once administered have by design a longterm effect. However, even the item most prone to degradation (i.e. the availability of the medical alert card) showed only minor loss rates. Additionally, we speculate that the promulgation of asplenia related information and distribution of medical alert cards via general practitioners might lead to secondary preventive effects in other patients with asplenia. Our data, however, preclude definite inferences in this area.
PSS is a rare event but nonetheless a major concern in asplenic patients [12], [21]. Although registry studies place the rate of PSS at 13/1000 person years of observation (PYO) [19], we were unable to detect an event of definite PSS in the intervention group of our cohort after three years of follow up (equivalent to 237 PYO). This might in part be due to the higher rate of preventive measures in our cohort. Importantly, though, we were unable to determine the cause of death in seven patients and an additional nine patients did not respond at all, which may have led to underdetection of PSS events.
Since this cohort was heavily influenced by the COVID-19 pandemic we sought to analyze the COVID-19-related outcomes of the participants. Although recommendations concerning vaccinations against COVID-19 were not incorporated in our intervention, the vast majority of participants received multiple vaccinations against SARS-CoV2. Somewhat surprisingly, the number of PCR-confirmed cases in our cohort is quite low but there is possibly some underreporting present due to decreased availability of PCR-tests in the later stages of the pandemic. Our study was not designed to allow for estimates of incidence of COVID-19 among asplenic patients, nevertheless we deem it noteworthy that there was only one case of severe COVID-19, which occurred before the widespread availability of vaccinations. Data regarding the outcome of COVID-19 in asplenic patients are still scarce and date either from very early in the pandemic [23] or rely mainly on self-reported health data [4]. Given the comparatively low incidence and benign clinical courses of COVID-19 observed in our cohort, however, our data do not indicate a propensity for severe COVID-19 among asplenic patients.
Our study has some limitations. While we tried to ascertain the status and, where applicable, cause of death of every participant by contacting general practitioners and next of kin, in some patients these questions could not be answered. Thus, our data may underestimate the occurrence of PSS in this cohort. However, in many cases which were lost to follow up, malignoma was already established at inclusion and seems a likely candidate for the reason of the loss to follow up. Additionally, due to the non-randomized design of our study we cannot rule out residual confounding. Although we used a well –designed statistical model to account for this, unmeasured confounding might still be present.
Our study also has several strengths. The use of the Health Action Process Approach (HAPA) theory for the intervention is innovative and emphasizes patient empowerment and motivation, which are critical for sustained behavioral change. The study’s design, incorporating a long-term follow-up of three years and the comparatively high follow-up completion rate provide robust insights into the durability of the intervention’s effects.
In conclusion, patients who had received our novel HAPA-based telephonic intervention exhibited significant and sustained improvement in adherence to guideline-based preventive measures. By emphasizing patient empowerment, our intervention may serve as a template for other preventive efforts aiming to increase long-term adherence to standard of care.

留言 (0)