
記住我


ANIT-induced cholestasis is a well-established animal model for studying the mechanisms of cholestasis. We therefore constructed in vitro and in vivo models of cholestasis by administering ANIT to rats and HepG2 cells.
Liver function indicators are of significant importance for the diagnosis and monitoring of diseases. ALT and AST are predominantly located in hepatocytes, and when elevated, they are typically indicative of hepatocyte damage. ALP and γ-GT serve as the most reliable indicators for the diagnosis of cholestasis, and when elevated, they are usually indicative of cholestasis or biliary tract disease. Elevated levels of TBA, TBIL and DBIL may serve as supplementary indications of cholestasis or hepatocellular dysfunction. The results of our research indicated that the expression levels of ALT, AST, ALP, TBIL, DBIL, TBA, and γ-GT were significantly elevated in the ANIT group in comparison to the Control group (P < 0.01). This indicated that ANIT caused hepatocyte dysfunction and cholestatic injury. However, the administration of PF was observed to significantly reverse the elevated levels of the aforementioned liver function indexes (P < 0.05) (Fig. 1A-G). These findings indicated that PF has the potential to significantly mitigate liver injury induced by ANIT. The accumulation of bile acids is regarded as the primary mechanism underlying cholestasis. The accumulation of toxic bile acids can lead to further inflammation, thereby exacerbating liver injury [14, 15]. Furthermore, the expression of inflammatory factors in the serum of rats was determined. The findings revealed that ANIT markedly elevated the expression levels of IL-1β, IL-6 and TNF-α in comparison to the Control group (P < 0.01) (Fig. 1H-J). In contrast, the HP group exhibited a notable reduction in the expression of these inflammatory factors in comparison to the ANIT group. Furthermore, Fig. 1L illustrated that the positive expression area of IL-1β in the HP group was markedly lower than that in the ANIT group. These findings indicated that PF may exert an inhibitory effect on the inflammatory response induced by ANIT. Furthermore, histological examination revealed that the ANIT group exhibited a significantly dilated confluent area, surrounded by augmented fibrotic tissue hyperplasia and inflammatory cell infiltration within the hyperplastic fibrotic tissue, in comparison to the Control group. Additionally, an increased number of bile duct epithelial cells were observed in the surrounding area, with the formation of some bile ducts. In comparison to the ANIT group, the hepatocytes in the HP group exhibited minimal signs of degeneration and necrosis. The local portal area demonstrated slight enlargement, while the fibrous tissue hyperplasia was reduced, accompanied by a minor infiltration of lymphocytes (Fig. 1K).
Fig. 1
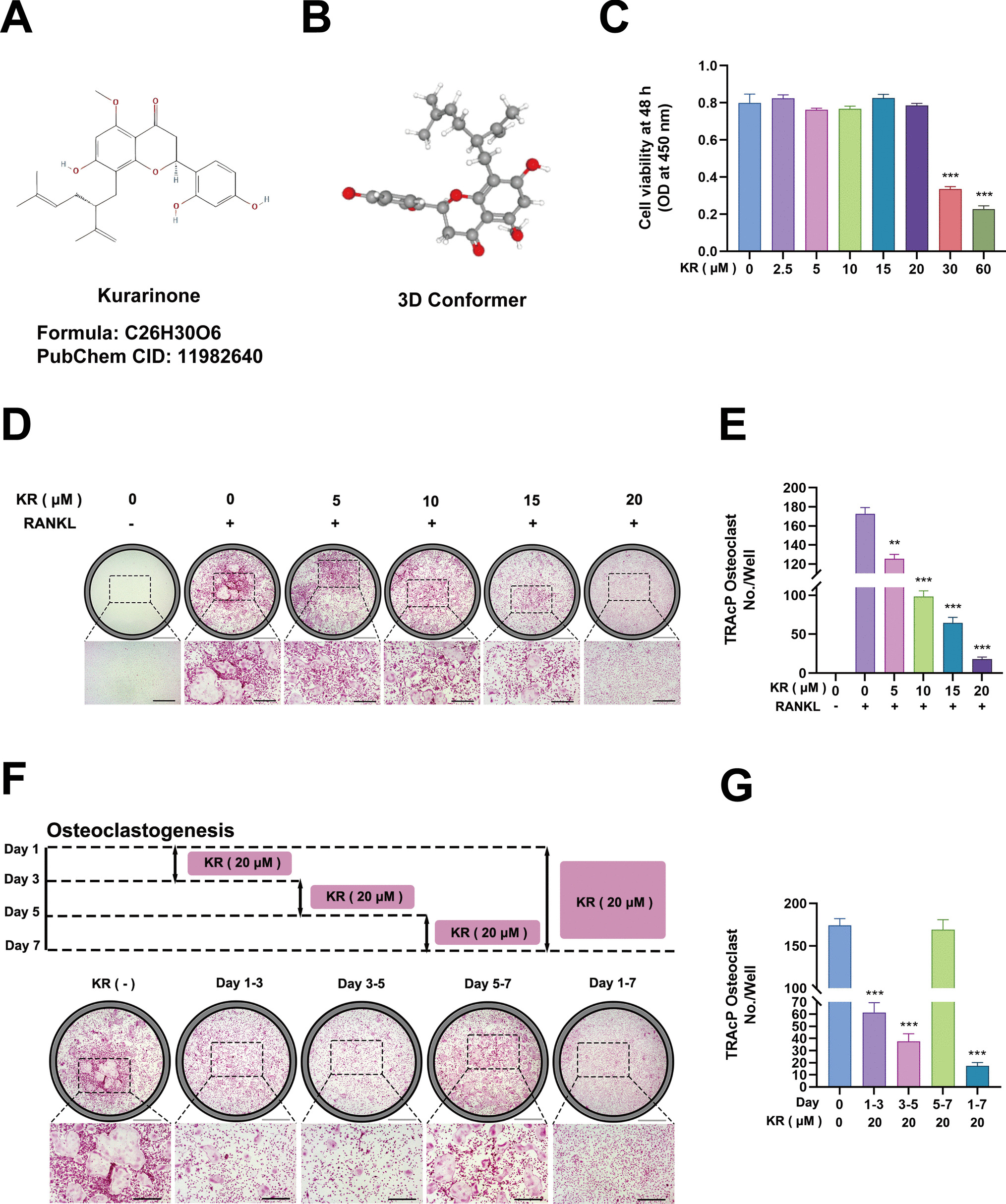
PF attenuated ANIT-induced cholestasis and hepatic injury. (A-G) The serum levels of ALT, AST, ALP, TBIL, DBIL, TBA and γ-GT were assessed. (H-J) Inflammatory cytokines (IL-1β, IL-6, and TNF-α) were quantified by ELISA. (K) Histopathological analysis was performed on liver tissues with H&E staining. (L) IL-1β expression in liver tissues was assessed by IHC. (M) Cytotoxicity assays were conducted on HepG2 cells to determine PF and ANIT doses. (N) A schematic representation of the in vitro experiment methodology was provided. (O) Cell viability was evaluated using CCK-8 assays post-ANIT exposure. All data are presented as mean ± SEM. ##P denotes a marked difference with respect to the Control group. *P < 0.05 and **P < 0.01 denote a statistically significant difference from the ANIT group
Fig. 2
PF inhibits apoptosis in vitro and in vivo to improve cholestasis. (A) TUNEL staining was performed to assess apoptosis in liver tissues. (B) TEM analysis was conducted on liver tissue ultrastructure. (C) Western blotting was used to detect Caspase 3 and Bcl-2/Bax ratio in liver tissues. (D) Immunofluorescence staining was performed for Caspase 9 in liver tissues. (E) Immunofluorescence staining was also conducted for Caspase 3 in liver tissues. (F) TEM analysis was carried out on HepG2 cell ultrastructure. (G) Western blotting was used to assess the active Caspase 3 and Bcl-2/Bax ratio in HepG2 cells. All data are presented as mean ± SEM. ##P denotes a marked difference with respect to the Control group. *P < 0.05 and **P < 0.01 denote a statistically significant difference from the ANIT group
In vitro experiments demonstrated that PF was not significantly toxic to HepG2 cells at doses of 0–30 μM. Cell survival was precisely 50% when ANIT was administered at 50 μM (Fig. 1M). Accordingly, the optimal modelling dose was determined to be 60 μM, while the therapeutic doses were set at 2.5, 5 and 10 μM. The administration and modelling of cells were conducted in accordance with the methodology illustrated in Fig. 1N. As illustrated in Fig. 1O, a high dose of PF (10 μM) markedly reversed the decline in cell survival resulting from ANIT (P < 0.01).
In conclusion, the in vivo experiments demonstrated that PF can reduce the expression of inflammatory factors by ameliorating the abnormalities of liver function and pathological tissue abnormalities caused by cholestasis and reducing the expression of inflammatory factors. in vitro experiments demonstrated that PF significantly enhanced cell viability.
PF Inhibited Apoptosis In Vitro and In Vivo to Improve CholestasisPrior research has indicated that PF attenuates the elevation of hepatic function markers and the discharge of inflammatory mediators elicited by ANIT. Our previous study demonstrated that PF could improve cholestasis by inhibiting the NLRP3/GSDMD classical pyroptosis pathway [5]. Furthermore, apoptosis and pyroptosis are closely linked and can regulate each other. For example, activation of Caspase1 in pyroptosis can also direct cells into Caspase3/9-dependent apoptosis. Therefore, we can further speculate whether PF ameliorates cholestatic liver injury by inhibiting apoptosis.
In our study, the percentage of apoptotic cells in liver tissue was quantified using fluorescence microscopy following TUNEL staining. The apoptosis rate in liver tissues was significantly elevated in the ANIT group compared to the Control group. However, apoptosis rates were reduced to varying degrees in the treatment groups (P < 0.05) (Fig. 2A). Ultrastructural analysis of liver tissue and HepG2 cells was conducted via TEM. in vivo experiments revealed pronounced abnormalities in the morphology and structure of hepatocytes in the ANIT group, characterized by round or irregularly shaped nuclei, prominent nucleoli, and heterochromatin aggregated around the nuclear membrane. Additionally, some mitochondria were slightly swollen, with lysed and fragmented cristae, and the loss of matrix granules. In contrast, hepatocytes in the PF-treated group exhibited more normal morphology and structure. The nuclei were oval, with prominent nucleoli and a more uniform chromatin distribution, predominantly euchromatin. Mitochondria displayed normal morphology and structure, with uniformly distributed matrix electron density, and the rough endoplasmic reticulum exhibited a normal appearance (Fig. 2B). In vitro experiments further demonstrated that HepG2 cells in the ANIT group exhibited clear signs of apoptosis, including reduced cell volume, mitochondrial wrinkling, expansion of the rough endoplasmic reticulum, and swelling of the Golgi apparatus. Conversely, in the PF-treated groups, particularly the 10 μM group, mitochondria and the rough endoplasmic reticulum appeared relatively intact, and no significant abnormalities in cell morphology and structure were observed (Fig. 2F).
We also examined the expression of apoptosis-related proteins. As shown in Fig. 2C and G, the expression of active Caspase 3 was significantly elevated in the ANIT group compared to the Control group, but this elevation was inhibited by PF treatment both in vivo and in vitro (P < 0.05). Additionally, the Bcl-2/Bax ratio was significantly lower in the ANIT group compared to the Control group (P < 0.05), suggesting that ANIT suppressed anti-apoptotic protein expression while promoting pro-apoptotic protein expression. However, treatment with PF significantly reversed the decrease in the Bcl-2/Bax ratio (P < 0.01). To further validate the expression of key apoptotic proteins, IF analysis was performed. In rat liver tissues, the fluorescence intensity of Caspase 9 and Caspase 3 was markedly higher in the ANIT group than in the Control group. PF treatment reduced the fluorescence intensity of both Caspase 9 and Caspase 3 (P < 0.05) (Fig. 2D-E).
These findings suggested that apoptosis may play a critical role in the progression of cholestatic liver injury, and that PF could inhibit ANIT-induced apoptosis. However, the specific signaling pathways through which PF modulates apoptosis warrant further investigation.
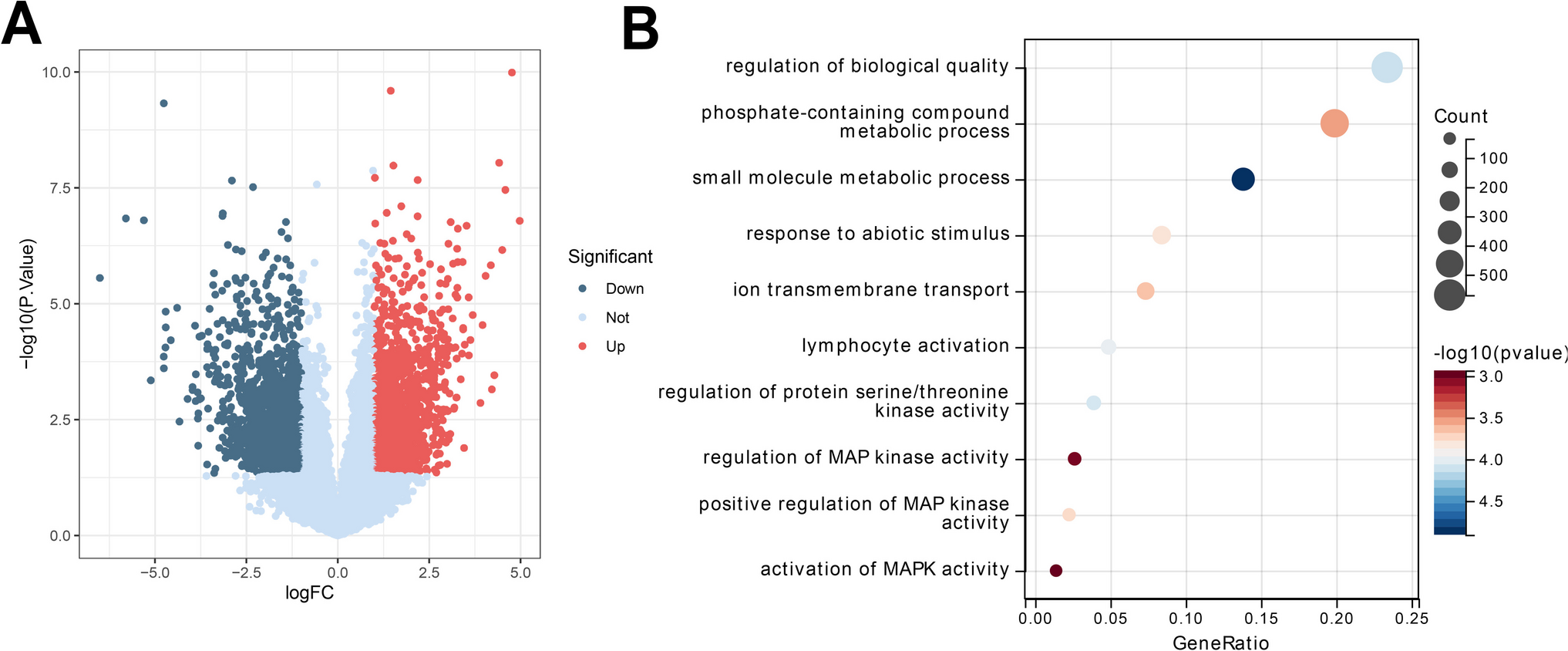
PF Targeted the JNK Signaling PathwayThe objective of this investigation is to ascertain the mechanism of action pathway through which PF specifically affects the onset of apoptosis. As illustrated in Fig. 3A, the PF was initially biotin-labelled and validated through mass spectrometry and NMR. Subsequently, the labelled PF was utilised to perform biological interactions with the HuProt™ 20 K Chip, with the aim of identifying effector proteins that can directly bind to PF (Fig. 3B). Following removing duplicates from the HuProt™ 20 K array search results, 625 PF targets were identified. Subsequently, 2,109 cholestatic targets were collated following the application of de-emphasis using the OMIM, GeneCards, and DrugBank databases. As illustrated in Fig. 3C, the Venn diagram depicts a total of 78 common targets. This diagram depicholestasised a network of drug-target-disease relationships involving PF, PF for cholestasis, and cholestasis for cholestasis, construcholestasised using Cytoscape software (Fig. 3D). The cross-targets of both PF and cholestasis were submitted to the STRING database for analysis, to identify protein–protein interacholestasision relationships between the targets. The Cytoscape software was employed for the visualization and topology analysis of the network parameters. The study’s findings indicated that MAPK8 was among the Top 10 most highly ranked targets. To ascertain the biological funcholestasisions of the principal targets of PF in the treatment of cholestasis, we conducholestasised GO and KEGG analyses on the aforementioned targets (Fig. 3E-F). The PPI networks of the pathway containing the MAPK8 target (Apoptosis) was illustrated in Fig. 3D. The Apoptosis pathway was among the Top 20 pathways in terms of the number of genes involved in the significant pathways and the significance in the KEGG results. The targets of the Apoptosis pathway enriched in KEGG results include MAPK9, MAPK8, FAS, FADD, BID. The PPI network of the Apoptosis pathway is illustrated in Fig. 3G. The evidence indicated that the Apoptosis pathway and cholestasis are highly correlated and that MAPK8 is a target with a high degree value. This suggested that MAPK8 was highly correlated with the apoptosis pathway and may be the promising target for improving cholestasis. Subsequent Chip analysis was conducted to gain further insight into the role of MAPK8 and MAPK9. Significant signal intensities were observed for both MAPK8 and MAPK9, indicating that PF exhibits a notable binding affinity for these proteins. The observed binding strength was found to be more pronounced for MAPK8 than for MAPK9 (Fig. 3H).
Fig. 3
PF targeted the JNK signaling pathway. (A) Biotin-labeling and validation of PF were performed using mass spectrometry and NMR. (B) A HuProt™ 20 K Chip assay was conducted to identify PF-binding proteins. (C) A Venn diagram showed the overlap between PF and cholestasis-related targets. (D) STRING database analysis was carried out on PPI networks, focusing on MAPK8. And Cytoscape was used for network visualization of drug-target-disease relationships. (E-F) GO and KEGG pathway analyses were conducted on identified targets. (G) The PPI network of the Apoptosis pathway showed specific enrichment targets. (H) Chip analysis was performed to assess PF binding to MAPK8 and MAPK9. All data are presented as mean ± SEM. ##P denotes a marked difference with respect to the Control group. *P < 0.05 and **P < 0.01 denote a statistically significant difference from the ANIT group
The aforementioned results indicated that PF may exert an influence on hepatocyte apoptosis through a direct interaction with MAPK8/9 (JNK1/2).
PF Mediated JNK Pathway to Improve Cholestasis by Influencing ApoptosisTo further substantiate the modulatory effect of PF on JNK, we conducted additional protein-level tests. The proteins of JNK and p-JNK were examined in vivo and in vitro by WB technique, and it was found that the values of p-JNK/JNK were significantly higher in the model group compared with the control group. Conversely, the administration of PF resulted in a notable improvement in this scenario (P < 0.05) (Fig. 4A). These findings indicate that PF markedly inhibits the activation of JNK induced by ANIT.
Fig. 4
PF mediated JNK pathway to improve cholestasis by influencing apoptosis. (A) Western blot analysis was performed to assess JNK and p-JNK levels. (B) Molecular docking analysis was conducted to evaluate PF binding to MAPK8. (C-I) Molecular dynamics simulation was carried out for the PF-MAPK8 complex. Analyses of hydrogen bonds, RMSD, RMSF, Rg, SASA, free energy landscapes, and MM/GBSA binding free energy were conducted for the PF-MAPK8 complex. All data are presented as mean ± SEM. ##P denotes a marked difference with respect to the Control group. *P < 0.05 and **P < 0.01 denote a statistically significant difference from the ANIT group
Furthermore, the interaction mechanism between PF and MAPK8 (JNK1) was investigated through the utilisation of molecular docking and molecular dynamics simulation techniques. Molecular simulation of the docking of target proteins and small molecules using AutoDock Vina v.1.2.5 software yielded a docking binding energy of −8.826 kcal/mol for the interaction between MAPK 8 and PF. PF was observed to significantly enhance the binding stability of MAPK 8 to PF through the formation of hydrogen bonding with several key amino acid residues of MAPK 8, thereby contributing to protein binding stability. The aforementioned key residues are Lys55, Tyr185, Gly38, and Ile32. These hydrogen bonding interactions contribute to the stable binding of PF and may also have an important impact on its biological activity (Fig. 4B). In light of the findings of the molecular docking analysis, the small molecule-protein receptor complexes were selected for 100 ns MDS in order to gain insight into the dynamic properties obtained by molecular docking. Firstly, the number of hydrogen bonds formed between the MAPK8 protein and PF exhibited considerable fluctuation during the simulation, with a predominant concentration between 3 and 6. This not only demonstrates that the hydrogen bonding interactions between the two are dynamic, but also reflects the complexity and flexibility of protein-small molecule interactions (Fig. 4C). The RMSD analysis revealed that the RMSD value of PF remained relatively stable between 20 and 100 ns, fluctuating between 0.10 nm and 0.15 nm. This indicates that the small molecule maintained a consistent structure throughout the simulation. The RMSF analysis also supported this finding, demonstrating that the MAPK8 protein exhibited stability in most regions during the simulation. However, at specific residue positions, such as It is evident that fluctuations are present at residues 100, 180, and 350, which may be indicative of flexible regions or functionally relevant active regions of the protein. Furthermore, the alterations in the radius of gyration and SASA substantiate the assertion that the protein preserves a relatively stable three-dimensional configuration throughout the simulation. In order to gain a deeper understanding of the dynamic behaviour and stability of the complexes, we mapped the three-dimensional free energy landscapes using the PC1 and PC2 derived from the principal component analysis (PCA) of the RMSD values and Rg values of MAPK8 and PF, in conjunction with the Gibbs relative free energy Z-axis, as the coordinate axes. The free energy landscape plots of MAPK8 with PF in both systems exhibited a single, sharp minimum energy cluster, indicating that the complexes remained highly stable throughout the simulation. In order to gain further insight into the degree of binding stability of small molecules to target protein receptor molecules, the MM/GBSA method was employed to calculate the binding free energy and amino acid residue free energy contributions (Fig. 4D-I). The findings suggest that PF exhibits a robust binding affinity for MAPK8.
PF Indirectly Inhibited Hepatocyte Apoptosis by Restoring Bile Duct BarrierBile duct epithelial cells are the primary cell type affected during the onset of cholestasis. Under normal physiological conditions, toxic components of bile, including bile salts and bilirubin, are efficiently excreted through the bile ducts. However, in the context of cholestasis, these substances accumulate abnormally within the bile ducts, exerting direct cytotoxic effects on cholangiocytes. Bile salts are particularly harmful as they can compromise cellular membrane integrity, leading to apoptosis or necrosis. Additionally, the excessive accumulation of bilirubin disrupts the normal metabolic functions of cholangiocytes, exacerbating bile duct injury. ANIT disrupts the structure and function of bile duct epithelial cells, resulting in the release of inflammatory mediators that attract the aggregation of inflammatory cells, including neutrophils and macrophages, which in turn leads to the development of inflammatory reactions in the vicinity of the bile ducts [6]. As a result of the obstructed bile flow, bile components such as bile salts, bilirubin, and cholesterol accumulate in the liver and bloodstream, leading to cholestasis [16]. The presence of elevated concentrations of bile salts in hepatocytes results in the induction of cellular damage, mitochondrial dysfunction, and oxidative stress [16, 17]. The continued accumulation of bile components and inflammatory responses can cause further damage to hepatocytes, leading to dysfunction and apoptosis. Prior research has demonstrated that PF can directly inhibit hepatocyte apoptosis by targeting the JNK pathway. The hepatobiliary microenvironment represents a significant impediment to bile accumulation. Consequently, we postulated that PF might inhibit the progression of cholestatic disease by directly inhibiting hepatocyte apoptosis and indirectly by restoring the biliary barrier in both directions.
In our study, HE staining of bile duct tissues revealed significant pathological changes in the ANIT group. The cholangiocytes exhibited disorganized arrangement, cytoplasmic vacuolization, and marked hyperplasia of small bile ducts. In contrast, cholangiocytes from the PF-treated group displayed more orderly arrangements, with a noticeable reduction in bile duct hyperplasia (Fig. 5A). Furthermore, as shown in Fig. 5B, cholangiocytes in the ANIT group demonstrated necrotic features, including mitochondrial swelling (disrupted cristae, loss of matrix, vacuolization), dilated endoplasmic reticulum (increased spacing between membranes), detachment of microvilli from the cell surface, cytosolic membrane damage, and leakage of cytoplasmic contents into the lumen. In contrast, the PF-treated group exhibited a dose-dependent improvement, with bile duct epithelial cells displaying more intact and well-preserved morphology and structure. The chromatin distribution was more homogeneous, the cytoplasm contained a higher number of mitochondria, some of which exhibited only mild swelling, and the rough endoplasmic reticulum showed slight dilation.
Fig. 5
PF improves bile duct injury induced by cholestasis. (A) H&E staining was performed on bile duct tissues. (B) TEM was used to examine the cholangiocyte ultrastructure. (C) TEM assessed tight junction integrity. (D-E) IHC was conducted for claudin-1 and ZO-1. All data are presented as mean ± SEM. ##P denotes a marked difference with respect to the Control group. *P < 0.05 and **P < 0.01 denote a statistically significant difference from the ANIT group
Bile duct epithelial cells, as specialized epithelial cells lining the bile ducts, play a crucial role in regulating bile production and maintaining bile homeostasis in vivo. Disruption of cholangiocyte function and bile duct integrity due to acute or chronic injury is closely associated with the accumulation of toxic bile acids, which in turn contributes to hepatic injury and inflammation [6]. Our study has demonstrated that ANIT may induce cholestasis by compromising the tight junctions of bile duct epithelial cells. Transmission electron microscopy revealed that, in the ANIT, the intercellular tight junction structures were disrupted, and cellular organization was markedly disordered compared to the Control group. Conversely, in the HP group, the cell membranes remained intact and continuous, with cells exhibiting tight and orderly arrangements, and the junctional complexes, including tight junctions, adherens junctions, and desmosomes, were well-preserved (Fig. 5C). Additionally, IHC analysis was conducted to assess the expression of tight junction-related proteins. As illustrated in Fig. 5D and E, the percentage of positive areas for claudin-1 and ZO-1 in rat bile duct tissues was significantly decreased in the ANIT group compared to the Control group, a reduction that was effectively reversed by PF treatment (P < 0.05).
In conclusion, PF ameliorated bile duct pathology and improved ANIT-damaged bile duct cell tightness and maintained the integrity of the connectivity complex to restore the bile duct barrier. Ultimately, it protected against ANIT-induced cholestatic bile duct injury.
留言 (0)