
記住我


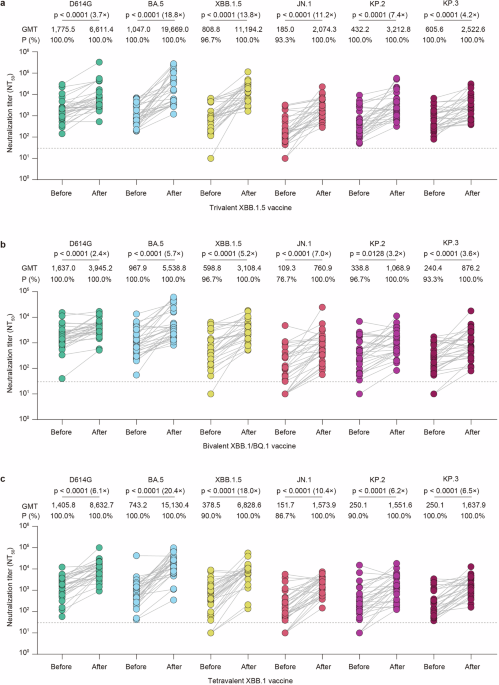
Between October 2020 and March 2022, a total of 129 patients from five hospitals were enroled in this study. After two cycles of neoadjuvant treatment, 62 patients (48.1%) were identified as MRI-responders and assigned to cohort A. Among the remaining 67 MRI non-responders, 26 patients continued with four additional cycles of docetaxel plus carboplatin and trastuzumab (TCbH; cohort B), while 41 patients received four cycles of TCbH in combination with pyrotinib (cohort C; Fig. 1).
Fig. 1
CONSORT diagram. Patients with HER2-positive breast cancer who received neoadjuvant therapy across five hospitals were assessed for eligibility. Breast magnetic resonance imaging (MRI) was performed at baseline, after every two cycles of neoadjuvant therapy, and prior to surgery. Early response was evaluated after the first two cycles of docetaxel plus carboplatin and trastuzumab (TCbH) treatment according to the Response Evaluation Criteria in Solid Tumours (RECIST) version 1.1. Responders continued with an additional four cycles of TCbH treatment (cohort A). Non-responders were further divided into cohorts B and C based on their preferences. Cohort B received four more cycles of neoadjuvant TCbH treatment, and cohort C received TCbH combined with oral pyrotinib for four cycles
As shown in Table 1, baseline demographic and disease characteristics were generally comparable across the study cohorts. A large proportion of patients enroled had stage II disease (62.6% in cohort A, 61.5% in cohort B, and 73.2% in cohort C, P = 0.57), hormone receptor (HR)-positive cancer (67.7% in cohort A, 76.9% in cohort B, and 61.0% in cohort C, P = 0.40), and Ki67 levels ≥20% (82.3% in cohort A, 73.1% in cohort B, and 78.0% in cohort C, P = 0.62). Additionally, HER2 protein 3+, as confirmed by immunohistochemistry (IHC), was prevalent across the study cohorts (88.7% in cohort A, 96.2% in cohort B, and 80.5% in cohort C, P = 0.16).
Table 1 Baseline characteristics of patients in the three cohorts stratified by MRI response and treatment regimensEfficacy analysisAll patients completed the planned six cycles of neoadjuvant therapy without experiencing disease progression, and subsequently proceeded to surgery. Among the MRI responders in cohort A, a total of 19 out of 62 patients achieved tpCR, resulting in a rate of 30.6% (95% confidence interval [CI]: 20.6–43.0%). Among the MRI non-responders, cohort C exhibited a higher tpCR rate of 29.3% (12 out of 41 patients, 95% CI: 17.6–44.5%) compared to cohort B, which had a rate of 15.4% (4 out of 26 patients, 95% CI: 6.2–33.5%). Similar trends were observed in exploratory analyses for the breast pathological complete response (bpCR) rate. The highest bpCR rate was found in cohort A at 38.7% (95% CI: 27.6–51.2%), followed by cohort C at 31.7% (95% CI: 19.6–47.0%), whereas cohort B had the lowest rate of 19.2% (95% CI: 8.5–37.9%; Fig. 2).
Fig. 2
Pathological complete response (pCR) in the intention-to-treat population according to magnetic resonance imaging (MRI) response and treatment assignment. Total pCR (tpCR, ypT0/isN0) and breast pCR (bpCR, ypT0/is) in the intention-to-treat population (N = 129), stratified by MRI response and treatment: Cohort A (MRI responders treated with docetaxel, carboplatin, and trastuzumab), Cohort B (MRI non-responders treated with docetaxel, carboplatin, and trastuzumab), and Cohort C (MRI non-responders treated with docetaxel, carboplatin, trastuzumab, and pyrotinib). The number (n) of patients who achieved pCR in a subgroup (N) are presented. The pCR rates were calculated with a 95% confidence interval (CI)
Subgroup analyses also suggested the differences in both tpCR and bpCR rates across the study cohorts, regardless of HR status, HER2 IHC status, TNM stage, Ki67 level and menopausal status. The rates were generally lower in patients with HR-positive breast cancer compared to those with HR-negative disease, regardless of treatment group (Supplementary Table 1).
As shown in Supplementary Fig. 1, after adjustment for age, menopausal status, HR status, HER2 IHC status, and Ki67 level, there was a non-significant trend indicating that cohort B exhibited a reduced likelihood of achieving tpCR (odds ratio [OR] = 0.40, 95% CI: 0.11 to 1.42) compared to cohort A, while cohort C showed a comparable likelihood of achieving tpCR (OR = 1.04, 95% CI: 0.40 to 2.70). Similar association patterns were observed regarding bpCR in the exploratory analyses (Supplementary Fig. 1). However, multivariable logistic regression analyses showed that no significant associations between clinicopathological variables and early response to neoadjuvant TCbH treatment (Supplementary Fig. 2).
With a median follow-up of 3.2 years, survival data remain immature, with only five disease-free survival (DFS) events recorded (three events in cohort A, one in cohort B, and one in cohort C): three visceral metastases, one axillary nodal recurrence, and one chest recurrence. No deaths were observed.
Safety analysisAdverse events (AEs) reported in all 129 patients are summarised in Table 2. In cohort C, which received pyrotinib in addition to TCbH treatment, the most common AEs were diarrhoea (24 out of 41 patients, 58.5%), erythropenia (19 patients, 46.3%), and anaemia (18 patients, 43.9%). Grade 3–4 AEs were rare, and no fatalities were reported. Furthermore, no patients had a left ventricular ejection fraction (LVEF) below 50%, nor did any experience a reduction greater than 10% from baseline prior to surgery. Among the 41 patients in cohort C, 13 (31.7%) required a pyrotinib dose reduction due to diarrhoea; however, no patients required dose reductions for docetaxel, carboplatin, trastuzumab, or pyrotinib for other reasons. These findings are consistent with previous clinical trials involving pyrotinib, where diarrhoea was the most frequently reported AE leading to dose reductions of pyrotinib.10,22
Table 2 Adverse events recorded in the NeoPaTHer trialaBiomarker analysisPre-treatment samples of tumour tissue and peripheral blood were collected from 70 patients, 37 of whom achieved a partial response after the initial 2 cycles of TCbH treatment, while 33 did not respond. Twelve patients, eight of whom had stable disease (non-responders), withdrew from the study after the initial treatment. Among the 58 patients included in the biomarker analysis, 33 patients were from cohort A, three from cohort B, and 22 patients from cohort C. Detailed characteristics of these patients are provided in Supplementary Tables 2 and 3.
The most frequent somatic mutations observed before treatment were TP53 (46/70 patients; 66%), PIK3CA (32/70; 46%), HMCN1 (6/70; 9%), ERBB2 (4/70; 6%), and BRCA2 (3/70; 4%). Co-mutations of TP53 and PIK3CA were present in 22 (31%) patients (Fig. 3). Non-responders showed higher frequencies of HMCN1 mutations (18.0% vs. 0.0%, P = 0.008) and BRCA2 mutations (9.0% vs. 0.0%, P = 0.10) compared to early responders (data not shown). Although the frequencies of TP53 and PI3KCA mutations were similar between responders and non-responders, patients with co-mutations of TP53 and PIK3CA were less likely to achieve an early partial response compared to those with single-gene mutations or no mutations (36.0% vs. 60.0%, P = 0.08) (Supplementary Fig. 3a). However, no significant difference in the tpCR rate was observed between patients with and without co-mutations (Supplementary Fig. 3b).
Fig. 3
Landscape of somatic single nucleotide variants in 70 patients with HER2-positive breast cancer, stratified by early response assessed using MRI after two cycles of neoadjuvant treatment. DNA sequencing was conducted using a custom-designed gene panel encompassing 769 frequently mutated genes in solid tumours. Gene mutations were analysed in relation to early response, which was assessed by MRI after the first two cycles of TCbH treatment according to the Response Evaluation Criteria in Solid Tumours (RECIST) version 1.1. Patients with a partial response (n = 37) were defined as those showing at least a 30% reduction in the sum of the longest diameters of all target lesions from baseline; patients not meeting this criterion were classified as having stable disease (n = 33). The types of gene mutations identified in each patient are annotated, with the mutation rate for each type presented on the left. Additionally, the status of pathological markers, including estrogen receptor (ER), progesterone receptor (PR), and HER2, as determined by immunohistochemistry (IHC), as well as menopause status and pyrotinib treatment, are also shown
Previous research has demonstrated that genetic mutational characteristics, such as tumour mutation burden (TMB) and genetic heterogeneity, serve as predictive biomarkers for cancer outcomes across various cancer types.23,24 However, in our study, no significant differences were observed in TMB (P = 0.19) or mutant allele tumour heterogeneity (MATH) scores (P = 0.09) between early responders and non-responders (Supplementary Fig. 4a, b). Nevertheless, patients with tpCR exhibited significantly higher TMB compared to those without tpCR (P = 0.01, Supplementary Fig. 4c).
Pathway analyses revealed that the frequency of mutations in the RTK-RAS pathway was significantly higher in the tpCR group compared to the non-tpCR group (56.0% vs. 21.0%, P = 0.02, data not shown). Multivariable logistic regression analysis, adjusted for MRI early response, TMB, RTK-RAS pathway mutation, and DNA damage response pathway mutation, revealed that TMB (OR = 5.38, 95% CI: 1.24–23.36, P = 0.03) and RTK-RAS pathway mutation (OR = 3.24, 95% CI: 0.82–12.77, P = 0.09) were associated with tpCR (Supplementary Table 4).
Stratified analyses based on the combined status of TMB and RTK-RAS pathway mutations revealed that patient responses were associated with both TMB levels and the presence of mutations in the RTK-RAS pathway (Supplementary Fig. 5). Patients with RTK-RAS mutations had a remarkable high tpCR rate, ranging from 40% to 60%, irrespective of TMB levels or the addition of pyrotinib (Fig. 4). In contrast, patients without RTK-RAS mutations and low TMB exhibited a significantly lower tpCR rate, with 0% (0/15) in those receiving trastuzumab and chemotherapy alone, compared to 8% (1/13) in those receiving additional pyrotinib to trastuzumab and chemotherapy (Fig. 4).
Fig. 4
Total pathological complete response (tpCR) rates in HER2-positive breast cancer patients, stratified by tumour mutation burden (TMB) levels, RTK-RAS pathway mutation status, and pyrotinib treatment. The tpCR and non-tpCR rates were calculated for patients who completed six cycles of neoadjuvant treatment with TCbH plus pyrotinib in cohort C (a) and those who received TCbH alone (no pyrotinib) in cohorts A and B (b). Stratification was based on the combined status of TMB levels (high or low) and RTK-RAS pathway mutations (wild-type or mutant). P values for each comparison are presented
留言 (0)