Trial oversight
This study received approval from the Ethics Committee at Changzhou NO.2 People’s Hospital Affiliated with Nanjing Medical University and was registered with the Chinese Clinical Trial Registry (ChiCTR2100050874,05/09/2021).
Participants
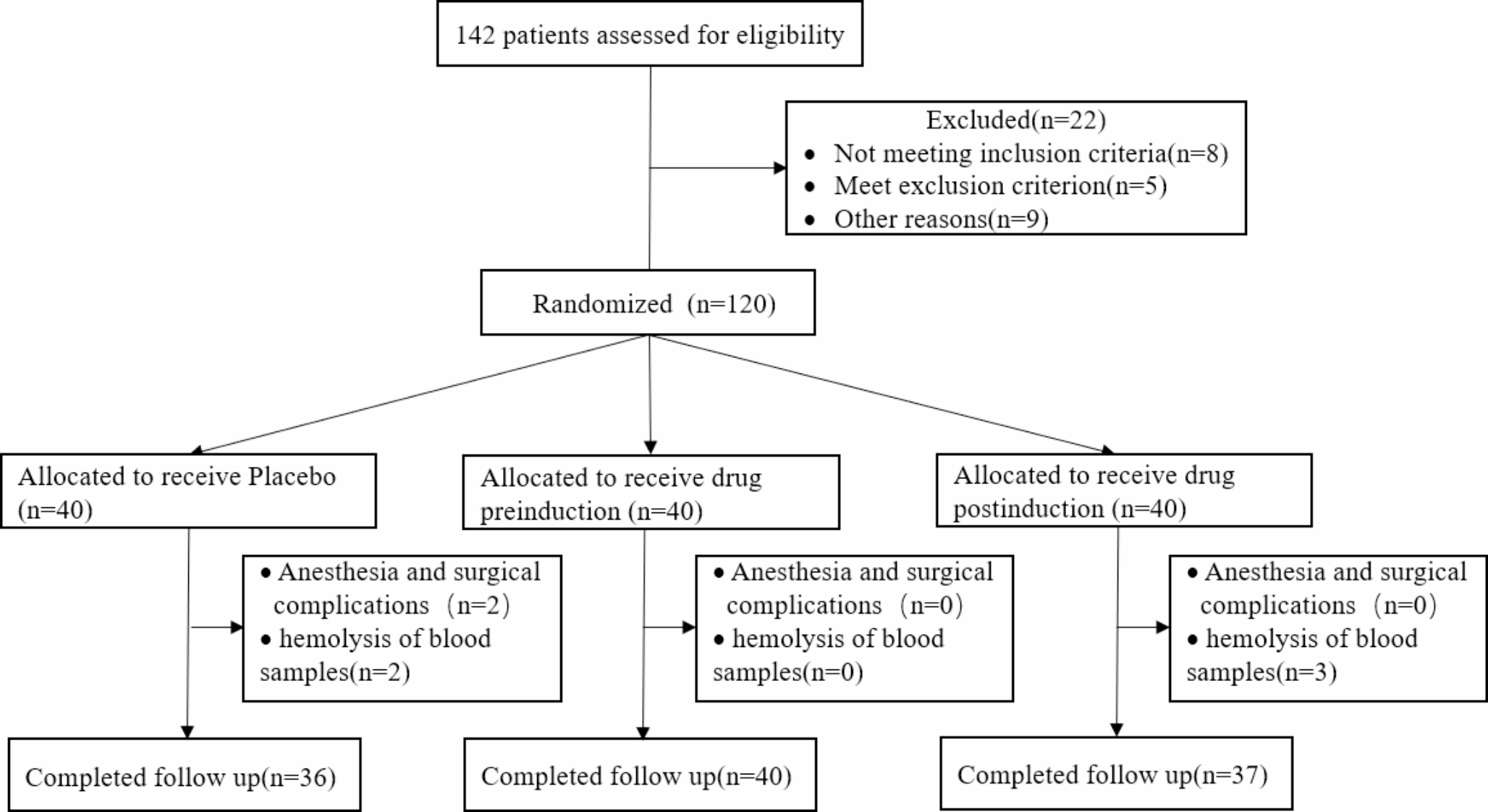
Prior to participating in the study, all 120 patients who underwent laparoscopic sleeve gastrectomy provided written informed consent. Eligible participants were between 18 and 60 years old, ASA physical status classification system class I or II, and had a BMI in the range of 32.5–45.5 kg/m2. Patients with a history of drug abuse, admitted to ICU with tubes, emesis, severe liver and kidney dysfunction, or mental illness were excluded from the study. The study took place at the NO.2 People’s Hospital in Changzhou between September 2021 and May 2023 and informed consent was obtained from all participants the day prior to their surgery, with the study conducted in the hospital’s operating rooms and wards.
Study procedures
A total of 120 eligible patients were divided into three groups using a random number table method, with each group comprising 40 patients. Anesthesiologists, the research team, and other trial staff were unaware of the allocation.
The randomization list was sent to the hospital pharmacy, which prepared 50 ml bags of study medication with identical appearances. Syringes were labeled with patient information, administration time, and route. Anesthesiologists, surgeons, and perioperative observers would be unable to discern whether the preparation was a control or experimental drug based on its appearance. To maintain blinding, emergency letters were prepared, each assigned to an opaque emergency envelope containing the drug number and name for unblinding and individual rescue in emergencies. After unblinding, corresponding cases would be considered dropout cases. Postoperative follow-up and data collection would be conducted by dedicated anesthesiologists. Patients, their families, anesthesiologists, surgeons, research recorders, and assessors would maintain confidentiality regarding group assignments and drug combinations. Individuals responsible for coordinating and supervising all aspects of the study would oversee the implementation of blinding to ensure the safety of participants and the reliability of results, aside from distributing emergency letters, protecting blind envelopes, and unblinding at the end of the study. Any adverse events spontaneously reported by patients or identified by researchers (such as psychiatric symptoms related to the study drug) would be carefully documented. Details would include the time of event occurrence, clinical manifestations, management, duration, and relationship to the administered drug. The association of adverse events with the intervention would be determined and summarized by the researchers. All serious adverse events would be registered and reported to the local medical ethics committee within 24 h.
In group Post-ESK, patients received an intravenous infusion of 0.2 mg/kg esketamine (No. 20060403; Jiangsu Hengrui Pharmaceutical Co., Ltd., Jiangsu, China) within 10 min after induction of anesthesia. In group Pre-ESK, the same dose of esketamine was intravenously infused, 2 h before the induction of anesthesia. In group Placebo, patients were given an intravenous infusion of 0.9% normal saline after the induction of anesthesia.
In this study, the effective management of anesthesia played a critical role in ensuring the safety and well-being of patients undergoing laparoscopic bariatric surgery. All patients received 400 ml of carbohydrate nutrient solution orally two hours before entering the operating room, and standard monitoring was initiated, including electrocardiogram, pulse oximetry, non-invasive blood pressure. Gastric ultrasound evaluation was performed by trained anesthesiologists before anesthesia induction. Anesthesia was induced using dexmedetomidine 1 µg/kg/h intravenously for ten minutes, and intubation was performed with 1.5-2 mg/kg propofol, 0.5 mg /kg sufentanil, 0.6 mg/kg rocuronium and 0.5 mg penehydine hydrochloride. Anesthesia was maintained by continuous intravenous infusion of 0.05–0.25 µg/kg/min remifentanil, 4-10 mg/kg/h propofol, 0.08 mg/kg/h cisatracurium besilate and continuous inhalation of 1-2% sevoflurane. Throughout the procedure, blood pressure, pulse oximetry, Bispectral Index (BIS), and end-tidal carbon dioxide (EtCO2) were closely monitored, blood pressure was controlled within ± 20% of the preoperative blood pressure, BIS was controlled between 40 and 60, and EtCO2 was maintained between 35 and 45 mmHg. 4 mg Tropisetron, 5 mg dexamethasone and 1.25 mg haloperidol were given intravenously to prevent postoperative nausea and vomiting (PONV). After surgery, the patient was sent to the Post anesthesia care unit (PACU) where they had to meet the Steward awakening score before returning to the ward. In the PACU, Transversus abdominis plane (TAP) block was performed under ultrasound guidance with 0.5% ropivacaine, and postoperative patient controlled intravenous analgesia (PCIA) was performed with 100 µg sufentanil, 20 mg oxycodone and 100 µg dexmedetomidine diluted with normal saline to100ml (continuous infusion rate of 2 ml/h. Single dose of 2 ml, lockout time of 15 min, maximum dose of 10 ml/h). All medication administration during the perioperative period was based on adjusted body weight, calculated using a specific formula (Adjusted Body Weight = Ideal Body Weight + 0.4(Actual Body Weight - Ideal Body Weight)).
Outcome measures
The primary outcome measures include the Patient Health Questionnaire-9 (PHQ-9) scores and plasma brain-derived neurotrophic factor (BDNF) concentration, with data collected on the day before surgery, the first day after surgery, and the second day after surgery.
The PHQ-9 is a simple, sensitive, and specific depression screening questionnaire consisting of 9 questions, based on the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders. The total score ranges from 0 to 27, where scores of 0–4 indicate no depressive symptoms, 5–9 indicate mild depressive symptoms, 10–14 indicate moderate depressive symptoms, and ≥ 15 indicate severe depressive symptoms.
Plasma BDNF levels were measured using the ELISA method, with venous blood samples collected on the day before surgery, the first day after surgery, and the second day after surgery between 8:00 and 10:00 am under fasting conditions. Participant venous blood was collected in anticoagulant-coated tubes. The samples were then kept at room temperature for 1 h, followed by centrifugation at 2000×g for 15 min. The resulting supernatant was separated and stored at -80 °C for further analysis. Plasma BDNF levels were determined using an ELISA kit (Elabscience) according to the manufacturer’s instructions.
The secondary outcome measures include: firstly, the Visual Analog Scale (VAS) pain scores (0 indicates no pain, 10 represents the worst imaginable pain), the number of times the analgesic pump is pressed, and the Postoperative Recovery Quality (QoR-15) scores, assessed on the first day after surgery and the second day after surgery; secondly, postoperative anesthesia and surgical recovery time; and thirdly, postoperative anesthesia-related complications as reported spontaneously by patients or identified by the researchers.
To enhance postoperative analgesia and reduce adverse reactions, various drugs are clinically used in combination for patient-controlled analgesia (PCA) therapy. Due to the diverse range of drugs involved, measuring a patient’s analgesic demand solely based on specific drug consumption poses challenges. Therefore, we used the number of presses on the PCA pump button to represent the patient’s analgesic demand. To ensure patient safety, the PCA pump has a lockout period, which is the interval between pressing the drug delivery button twice, preventing accidental overdosing due to repeated administration. Pressing the “PCA button” during the lockout period does not result in a single dose, and such presses are considered “invalid presses.” The number of PCA pump presses and valid presses can better reflect a patient’s analgesic demand. QoR-15 assesses overall patient satisfaction with postoperative recovery.
Statistical analysis
Data analysis was conducted using SPSS 25.0 software package, with a significance level set at p = 0.05. Categorical data were presented as numbers and percentages, while continuous data were expressed as means and standard deviations (SD). We utilized repeated measures analysis of variance (ANOVA) to analyze changes in PHQ-9 scores and plasma BDNF concentrations from preoperative day 1 (baseline) to postoperative day 2. Between-group comparisons of other continuous variables were conducted using one-way ANOVA with Bonferroni correction, while categorical variables were assessed using χ² tests or Fisher’s exact tests. Binary logistic regression analysis was employed to compare pre- and postoperative predictive factors between patients with and without postoperative depressive symptoms. After screening, baseline PHQ-9 scores, baseline and postoperative day 1 plasma BDNF levels, as well as postoperative day 1 VAS scores, PCA pump presses, and valid presses were included as covariates in this model. Pearson linear correlation was used to explore the linear relationship between plasma BDNF levels and postoperative depressive symptoms. Due to the low incidence of depressive symptoms on the second postoperative day, binary logistic regression analysis was not conducted for this period.




留言 (0)