
記住我



We aimed to enroll at least 20 participants to assess feasibility, participant satisfaction, and potential challenges of delivering this novel intervention, as well as preliminary data on outcomes of the intervention on pain and related symptoms. We recruited from August 7–29, 2023 by first contacting Veterans who participated in other studies related to cannabis use and chronic pain, including a qualitative study (Bergmans 2024) and a longitudinal registry called MIVetsCan. We also recruited participants by posting on the University of Michigan’s research website (UMHealthResearch.org). The last study assessment was completed on December 5, 2023.
Participants were adults aged 18 or older who were Armed Services Veterans with self-reported chronic pain lasting 3 or more months and were interested in using or currently using cannabis for chronic pain management.
Participants completed informed consent documents electronically using the MyDataHelps app (CareEvolution, Ann Arbor, MI), which provides a secure platform for collecting protected health information remotely and has been used in large well-known studies such as the NIH All of Us Study and the eFramingham study (Quer et al. 2021; Pathiravasan et al. 2021; Lin et al. 2020; McManus et al. 2019). In addition to informed consent, the MyDataHelps app served as the vehicle for data collection via study questionnaires and synced activity tracking devices (i.e., Fitbits) as well as automated study notifications. The app also displayed a digital dashboard so that participants could track changes in their pain-related symptoms and cannabis use over time.
The University of Michigan Institutional Review Board (IRB) approved all study methods and procedures under HUM00231159. Participants received up to $200 for participating in the study, with payment disbursed after each completed survey. This trial was registered to clinicaltrials.gov as NCT06320470.
Intervention developmentWe developed the educational intervention with insight from multiple sources, including the most recent and relevant scientific literature (Bell 2023; Bhaskar 2021; MacCallum 2018; National Academies of Sciences, Engineering, and Medicine 2017; Boehnke et al. 2024), consultation from a medical cannabis expert who had substantial clinical experience working with medical cannabis patients (co-author EL), input from Veterans via a Community Advisory Board (CAB), and informed by the tenets of Motivational Interviewing (MI). We developed a manual for this intervention, drawing from several comprehensive reviews on the effects of cannabinoids and how they related to chronic pain symptoms (Bell 2023; Bhaskar 2021; MacCallum 2018; National Academies of Sciences E, and Medicine 2017). Two Master’s-level therapists (GB, DH) delivered the intervention to study participants. Required hiring criteria for this role included past training and experience with client therapy, manualized intervention delivery, and MI. The last criterion was derived from the study team’s history with conducting motivational interviewing-based interventions in previous studies (Bohnert et al. 2016; Blow et al. 2017).
To center Veterans’ perspectives, we used a community-engaged approach throughout the study design process. These efforts included soliciting feedback from the Ann Arbor Veteran Affairs Veterans Research Engagement Council (VREC) and establishing a Community Advisory Board (CAB) to help shape research priorities, including providing input on study design and educational materials. The CAB is primarily composed of Veterans who have chronic pain, representatives of organizations that provide services to Veterans, as well as medical providers who work with Veterans. The CAB influenced the development of the intervention by helping us to ensure its relevance to Veteran communities and verifying that the design was responsive to Veteran priorities and perspectives. For example, we modified the coaching intervention to add extra information related to cannabis product safety, dosing, and cannabis legality based on the CAB’s feedback. We also sought feedback and approval for our recruitment materials and approach with the CAB and VREC, who suggested additional opportunities and settings for engaging with Veterans such as Veteran resource fairs.
We designed a manual for the coaching intervention that draws from the cannabis literature as well as the spirit and guidelines of MI. MI is an evidence-based, person-centered approach that helps to spur behavioral change through opportunistic conversing rather than prescribed or directed recommendations (Miller 2012). MI encourages a curious, non-hierarchical, and non-judgmental conversational style in which the coach supports and affirms participant autonomy. The delivery of a MI-based coaching intervention is fundamentally relational: coaches demonstrate partnership, convey acceptance, cultivate compassion, and emphasize empowerment. In addition to borrowing from the humanistic philosophies of MI, we directly incorporated MI-specific skills and tasks into the intervention: open questions, affirmations, reflections, and summaries. Coaches use each as conversational vehicles to favor participant language for change versus the status quo. Open-ended questions are featured prominently in the didactic portions of the manual, such as the “elicit-provide-elicit” structure to first explore what the participant already knows, then requesting permission to share relevant interviewer knowledge, and finally exploring the participant's response. Coaches then selected salient elements from participant speech to reflect back as a demonstration of active listening. More complex reflections include sharing coach observations about participant’s nonverbal cues or hypotheses about what the client may be feeling or thinking but have not explicitly shared. Reflections impart a sense of empathy and build rapport. The spirit and tasks of MI informed the style in which the standardized manual was delivered to participants; coaches identified relevant MI skills to use within each section to ensure participant engagement, partnership, and empowerment. The manual was unscripted to allow the coaches therapeutic creativity on connecting the content to the individual participant and their lived experiences (e.g., cannabis naïve, their specific pain symptoms, etc.).
Our goal was to empower participants with sound scientific information via encouraging partnerships to achieve confidence in pain symptom self-management with self-selected medical cannabis products. Participants met with the same coach (GB or DH) throughout the trial to enable relationship-building with ample validation and support in the process of change. Further, the coaching intervention was consistently adaptive to participant feedback. During each, we asked participants to rate their confidence in using cannabis for pain management on a 0–10 scale (0 = not at all confident, 10 = completely confident) Likert scale. Coaches then explored what made the participant choose their rating, why the rating was not lower (e.g., a 6 rather than a 4), and whether the participant could identify factors that might increase their confidence in the future. Discrepancies between the selected number and other statements made by participants were also explored, such as a low number coupled with a demonstrated high degree of competence or vice versa. With safety, accuracy, and empowerment in mind, coaches identified and addressed misinformation or discouragement.
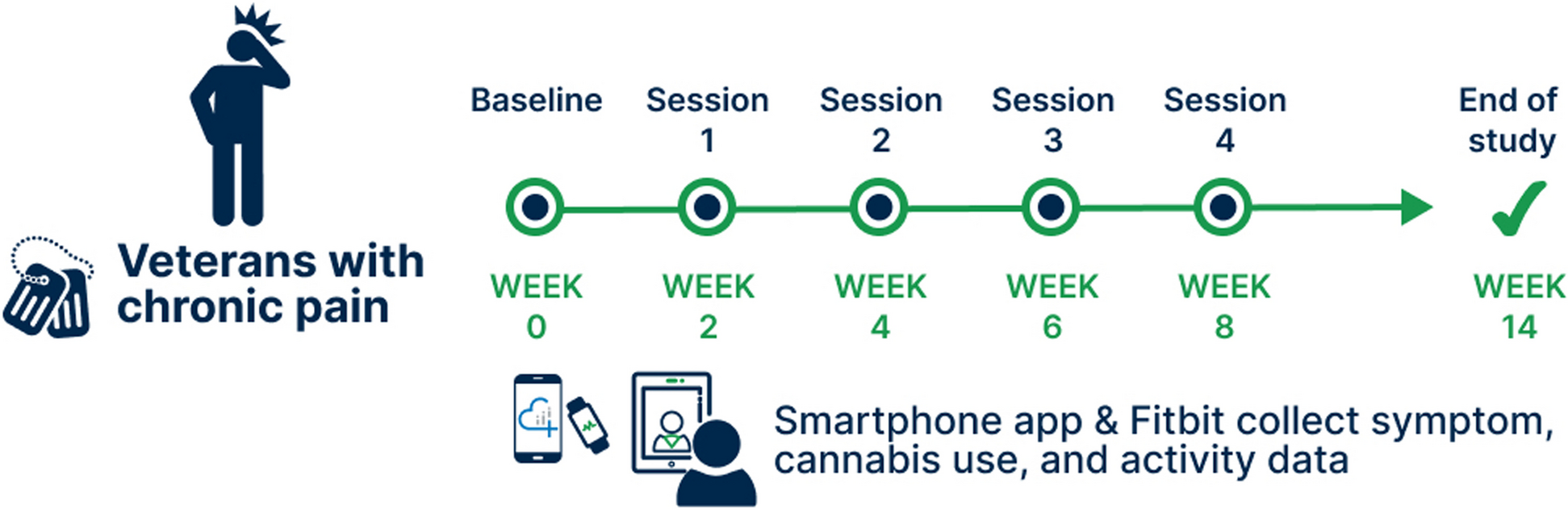
Intervention description and deliveryFigure 1 provides an overview of the study design. In brief, this 14-week long intervention encompassed 4 cannabis coaching visits and access to educational materials about cannabis. After enrollment, we gave study participants access to the Cannabis Guide, which is a set of infographics delineating steps for using cannabis products to achieve pain management goals aligned with expert guidance published in the scientific literature (Bell 2023; Bhaskar 2021; MacCallum 2018; Boehnke et al. 2024). The Cannabis Guide briefly summarizes key didactic elements from the manual. We then assigned participants to a cannabis coach who offered up to 4 virtual coaching sessions scheduled approximately 2 weeks apart. We followed participants for 6 weeks after the final coaching session, with the primary endpoint assessments occurring at 14 weeks after baseline.
Fig. 1 Coaching session content (overviewed in Table 1)Table 1 Overview of manualized intervention
Coaching session content (overviewed in Table 1)Table 1 Overview of manualized interventionThe first coaching session was on average 57.8 min (SD = 9.9 min) and resembled an “intake” visit. Coaches asked participants to provide detailed information on their cannabis use history, pain experience and symptoms, as well as co-occurring issues such as anxiety and sleep problems. Accurate histories enabled coaches to tailor cannabis plans to each participant’s set of symptoms and previous helpful or unhelpful experiences with cannabis therapeutics. The coaches also asked participants to share relevant health-related goals that they hoped to achieve through cannabis-based treatment. These goals served as useful signposts for coaches to revisit over the course of the intervention, and included stress management, sleeping well, better pain control, reduction in side effects, going back to school, and better relationships with others.
Once coaches collected histories, noted goals, and began to develop rapport with participants, they moved onto the didactic portion of the first session: the domains of cannabis use. Referencing the Cannabis Guide, coaches used the motivational interviewing task of “elicit-provide-elicit” with the following topics to partner with participants increase their understanding of cannabis products: differential effects of THC and CBD, routes of administration available (i.e. smoking, vaporizing, eating, topicals, tinctures) and how their effect onsets and durations differ, methodical “start low, go slow” dosing strategy, effective timing of use (aligning therapeutic effect with onset of symptoms), safety considerations, and side effects. This task allowed coaches to learn what all participants, regardless of their history of cannabis use, already knew about each clinical pearl before providing information to fill in any gaps or correct misinformation. This also helped coaches to optimize their time with participants by reducing redundant didactics. The coaches then partnered with the participants to come up with a realistic cannabis use plan given the participant’s pain symptoms, their history of cannabis use, their health goals, and what was realistic to integrate into their lives. The coaches encouraged tracking symptoms and cannabis use via MyDataHelps so that this information could inform participant choices about current and future cannabis use. The first session concluded with coaches collaborating with participants to decide the appropriate first steps in optimizing their use (Fig. 2).
Fig. 2
Example post-visit summary email from coach to a study participant who reported daily back and knee pain, current use of smoked cannabis (THC), and desire to experiment with alternate routes of administration
The three following sessions served to reinforce content from the first session, address any concerns that arose since the last session, and discuss potential changes to the self-directed treatment approach (mean duration = 30.3 min; SD = 7.8 min). Coaches encouraged participants to share any behavioral changes related to cannabis use, the status of their pain symptoms, and side effects. In the spirit of patient-centered care, coaches provided individualized guidance reflective of each participant’s goals, needs, and limitations. For instance, some participants wanted to experiment with CBD products only. Some did not want to smoke or vaporize, but rather focus on ingestion, tinctures, or topicals. Others felt the most relevant goal was to address insomnia, which exacerbated their pain symptoms during the day. The final session mimicked other follow-up sessions, but additionally included dialogue about how participants could independently adjust and monitor their use routines post intervention, identifying supports and lessons learned.
留言 (0)