Participants
This was a retrospective chart review. Patients were eligible for this study if they had been referred to the Johns Hopkins Chronic Fatigue Clinic between January 2020 and July 2023, and (a) they reported difficulty maintaining arms-overhead or arms-extended postures, and (b) their clinical examination had included an abbreviated one-minute EAST (see below). We excluded those who had undergone surgery in the upper limb, neck, or skull base, as this could have affected the symptoms reported during the EAST.
Diagnostic criteria
ME/CFS: We classified individuals as having ME/CFS if they satisfied the 2015 IOM definition [1], which required the following core symptoms: (1) a substantial impairment in the ability to engage in pre-illness levels of occupational, educational, social, or personal activities, persisting for more than 6 months, accompanied by profound, novel fatigue that is not the result of ongoing excessive exertion and is not substantially alleviated by rest, (2) post-exertional malaise, (3) unrefreshing sleep, and either (4a) cognitive impairment or (4b) orthostatic intolerance. We defined idiopathic chronic fatigue as fatigue that lasted at least 6 months but did not meet the IOM criteria.
Orthostatic Intolerance: We classified patients as having orthostatic intolerance if they had had frequent orthostatic symptoms in the absence of hemodynamic abnormalities, or if they had been diagnosed with neurally mediated hypotension (NMH) or postural tachycardia syndrome (POTS) using either a head-up tilt table test or a passive standing test. The diagnosis of NMH required a sudden and sustained drop in systolic blood pressure of at least 25 mm Hg compared to the supine values, with no associated increase in heart rate, and accompanied by symptoms of presyncope (severe lightheadedness, weakness, nausea, or diaphoresis) [24]. The diagnosis of POTS for those 12–19 years required at least a 40-beat increase in heart rate compared to supine values over 10 min of standing or head-up tilt testing, with chronic orthostatic symptoms, and without orthostatic hypotension within the first 3 min. For those 20 years and older, a 30-beat increase was sufficient for the diagnosis. [25]
Joint Hypermobility/Ehlers-Danlos syndrome: At the initial visit in all patients referred to the Chronic Fatigue Clinic, we routinely obtain a 9-point Beighton score to screen for joint hypermobility, using a goniometer for measuring joint angles [26]. For the Beighton score, an examiner assigns one point on each side of the body for (a) passive dorsiflexion of the 5th finger at the metacarpophalangeal joint of > 90 degrees, (b) passive apposition of the thumb to the flexor aspect of the forearm, (c) extension of the elbow > 190 degrees, (d) extension of the knee > 190 degrees. The 9th point is for the ability to place the palms flat on the floor while bending over at the waist without bending the knees. In previous work, we had used the Beighton cut-off score of ≥ 4 to indicate joint hypermobility, and used the same cut-off in this study as well [5]. By definition, individuals diagnosed with Ehlers-Danlos syndrome were included as having joint hypermobility. We did not perform genetic testing to confirm the diagnosis of Ehlers-Danlos syndrome (EDS), as there is no known genetic mutation for the most common type of EDS (hypermobile EDS).
Study procedures
Modified EAST procedure: Patients were seated in a chair, with their feet on the floor, back supported, and arms in a “hands up” or “candlestick” position (meaning the arms were abducted to a 90-degree angle in the frontal plane, with forearms vertical and palms forward). Patients were instructed to then open and close their hands every 2–3 s repeatedly for 1 min (rather than the customary 3 min). The 1-min duration has been used by others [27], and was chosen to reduce the likelihood of provoking prolonged ME/CFS symptoms following the test.
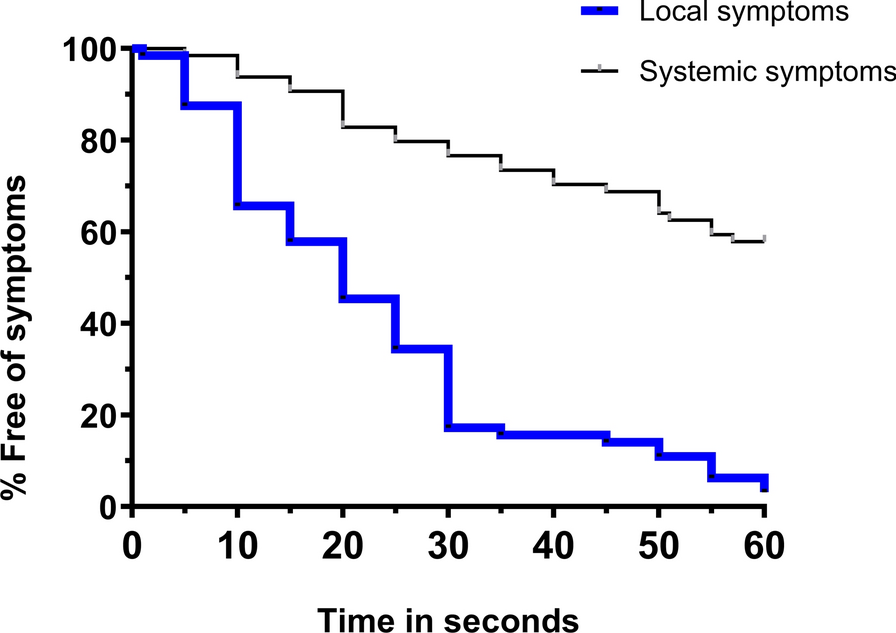
Patients were asked to report to the examiner as soon as they experienced the onset of any symptom in the upper limbs or any symptom in general. The test was considered abnormal for local symptoms if the participant experienced pain, fatigue, heaviness, paresthesias, warmth or tremulousness in the upper limb, shoulder, neck, head or upper back. The test was considered abnormal for systemic symptoms if the participant experienced overall fatigue, cognitive fogginess, lightheadedness, racing heart, diaphoresis, dyspnea, overall warmth, and nausea. We calculated the overall prevalence of abnormal EAST tests as those with either an abnormal local or an abnormal systemic test. Patients were permitted to stop the test at their discretion if their symptoms exceeded their own level of comfort.
Upper limb neurodynamic test 1 (ULNT1): Based on earlier experience, we routinely perform an upper limb neurodynamic test 1 (ULNT1, often termed the upper limb tension test), in accordance with the method described by Butler [28]. With the patient positioned supine and facing forward, arms at the sides and with legs together and knees extended, the examiner then performs the following sequence of maneuvers: a) abduction of one of the subject’s arms to 110 degrees while the shoulder girdle is held in a depressed, but neutral position of glenohumeral rotation, with the elbow flexed to 90 degrees, b) supination of the forearm with wrist, thumb, and finger extension, c), lateral rotation of the arm to 90 degrees, d) elbow extension to the point at which the subject reports stretch along the upper limb, e) contralateral neck side bend to bring the ear close to the contralateral shoulder, with the head facing forward (looking up at the ceiling), f) ipsilateral neck side bend toward the shoulder of the limb being tested, again with the head facing forward. Full elbow extension is measured as 180 degrees. An abnormal range of motion on this test consists of an elbow angle less than 170 degrees at the onset of stretch in one or both arms. An abnormal symptomatic response consists of provocation of symptoms other than stretch in the anterior shoulder or antecubital fossa or paresthesias in the hand (e.g., discomfort in the back, neck, or head, or lightheadedness).
Statistical analysis
We used descriptive statistics, including mean (SD) or median and interquartile range (IQR) where appropriate. We calculated the time until the onset of local upper limb as well as systemic symptoms using survival curves. To explore the influence of joint hypermobility on the provocation of symptoms, we compared the survival curves in hypermobile versus non-hypermobile patients using the log rank (Mantel-Cox) test (GraphPad Prism, version 10.3; GraphPad Software, La Jolla, California, USA; www.graphpad.com).






留言 (0)