
記住我
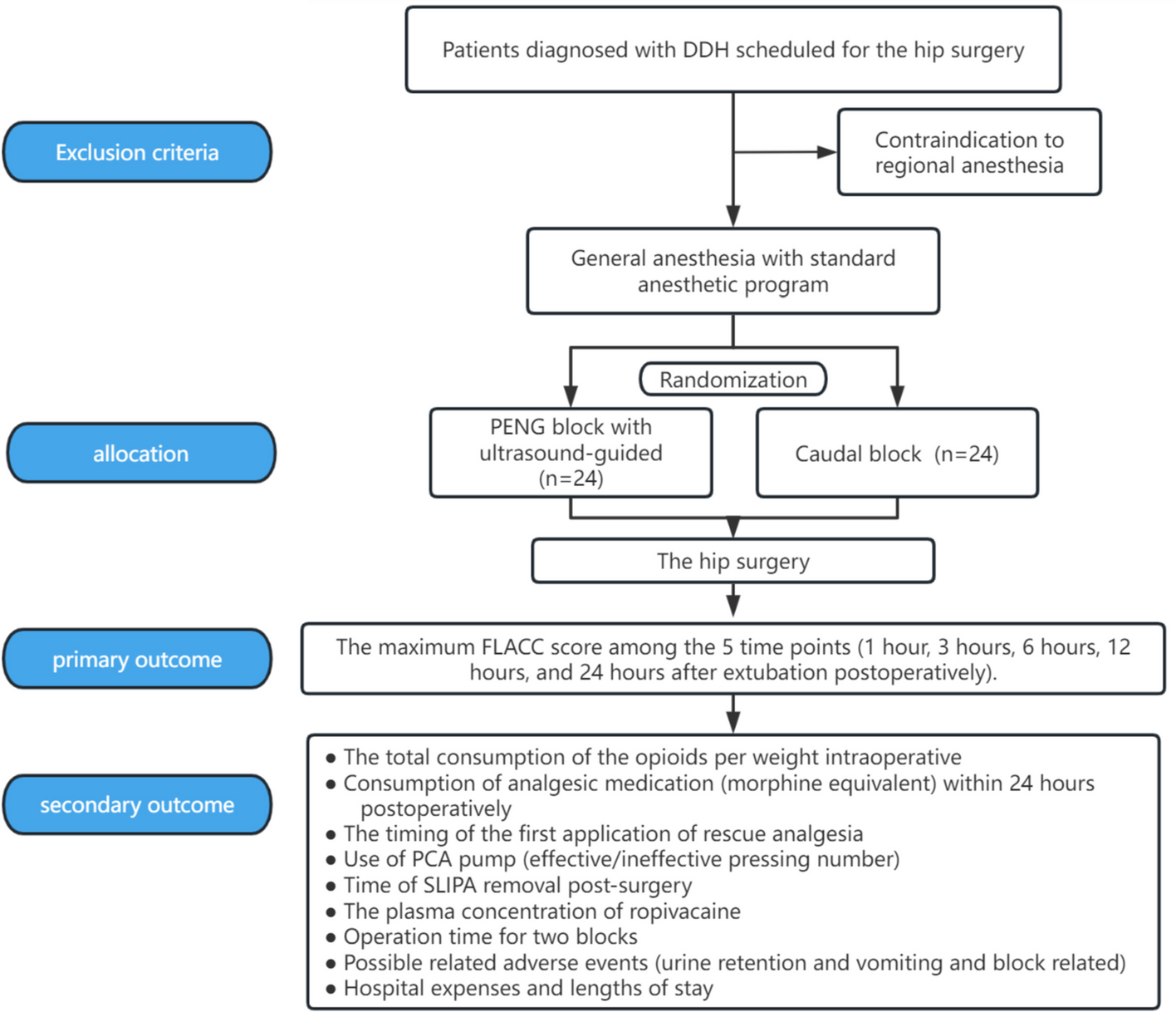


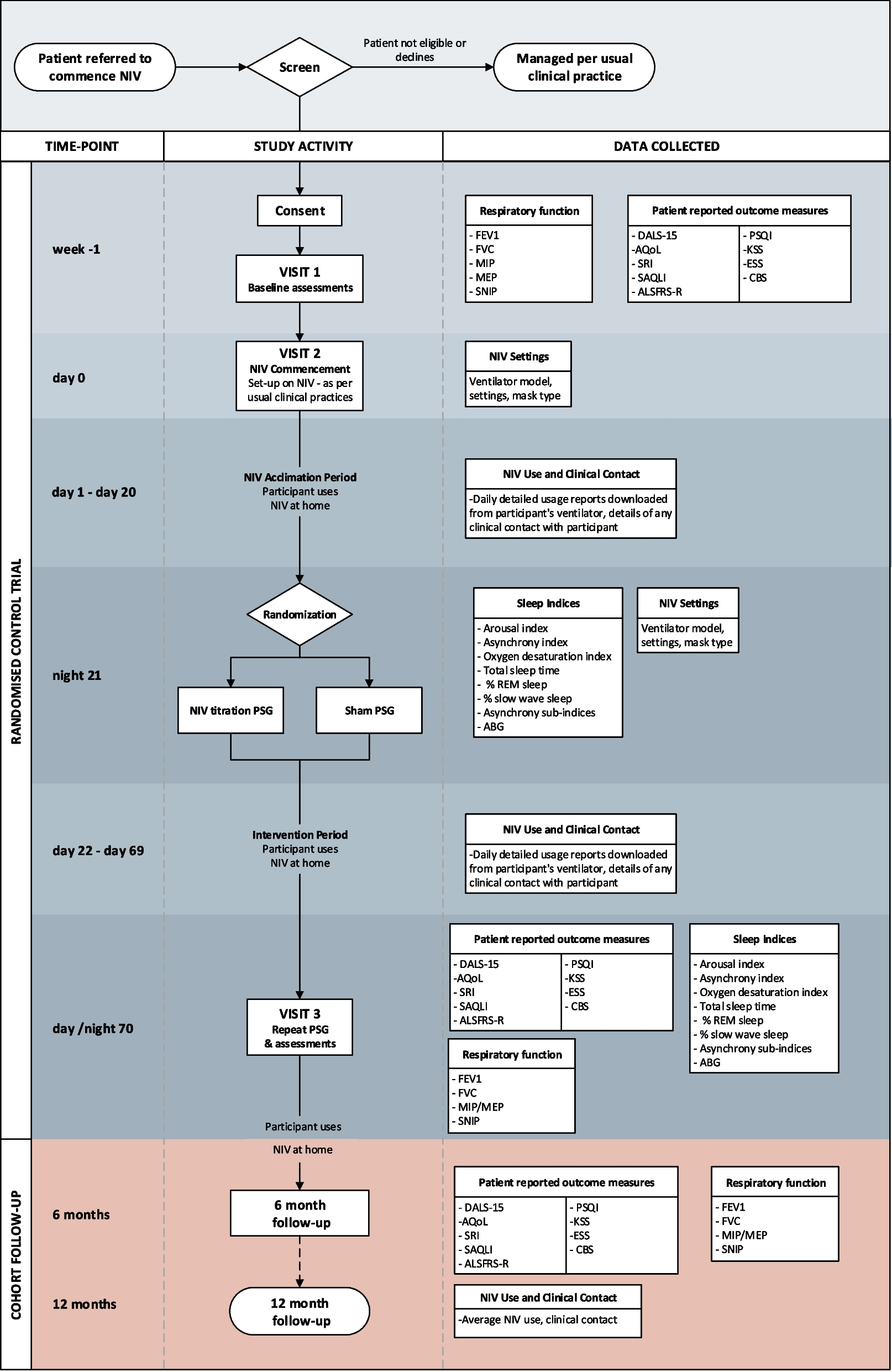
A prospective, double-blind, randomized, single-center non-inferiority parallel-group 2-arm study with a 1:1 allocation ratio was conducted at West China Hospital in China. Figure 1 depicts the study flow chart, and the protocol corresponds to the SPIRIT 2013 statement [16]. Table 1 shows the participant timeline for patient enrollment and assessment.
Fig. 1
The flow chart of this study. DDH, developmental dysplasia of the hip; PENG, pericapsular nerve group; FLACC, face, leg, activity, cry, consolability; PCA, patient-controlled analgesia; SLIPA, pharyngeal airway
Table 1 The participant timeline. PACU, post-anesthesia care unit; FLACC, face, leg, activity, cry, consolability; PCA, patient-controlled analgesia Ethics and disseminationThe Ethics Committee on Biomedical Research, West China Hospital of Sichuan University approved the study on January 13, 2022 (2021–1607). The study was registered with the Chinese Clinical Trial Registry (ChiCTR2100053128) on 12 November, 2021. The study findings will be published in peer-reviewed journals.
Participant and informed consentAn impartial investigator will undertake recruitment on the ward 1 day before surgery, based on pre-defined inclusion and exclusion criteria. Table 2 summarizes the study’s eligibility requirements. The investigator will describe the study’s objective, procedures, benefits, and potential risks to participants’ guardians before obtaining informed permission. Guardians have access to all relevant information throughout the trial period and may revoke their consent at any moment. We have not implemented any additional measures to promote participant retention.
Table 2 Inclusion and exclusion criteria of the study Randomization and blindingA random number produced by Excel will be used to assign patients to either the caudal block or PENG block groups, with a 1:1 allocation ratio maintained. The group assignment for each member will be sealed in an envelope. The randomization process will be conducted by an independent statistician who will not involve in data analysis. Individual anesthesiologists will provide regional anesthesia (he will not take part in management of perioperative period and follow-up visit), and a specialized anesthesiologist in charge of monitor intraoperative care, while postoperative follow-up researchers will be barred from accessing the operating room. Allocation blinding will be maintained for the anesthesiologists (in charge of intraoperative care and follow-up), participants, surgeons, and statisticians will all be allocated blind until the final analyses are completed. Unless a research-related serious adverse event occurs, the principal investigator will report any unblinding immediately if necessary; otherwise, we will not unblind.
InterventionsAll participants will be given general anesthesia using our standard anesthetic program, while an experienced anesthesiologist will administer regional anesthesia and a designated pediatric surgeon will perform surgical procedures using the same technique. All medications were administered in accordance with the protocol; no concomitant medications were allowed in our study.
All patients are subjected to standard electrocardiography, pulse oximetry, and noninvasive blood pressure monitoring as soon as they reach the operation room. To ease insertion of a streamlined liner of the pharyngeal airway (SLIPA), both groups receive conventional general anesthesia consisting of intravenous midazolam 0.05 mg·kg−1, sufentanil 0.3–0.5 µg·kg−1, propofol 2–3 mg·kg−1, and cis-atracurium0.1–0.2 mg kg−1. Anesthesiologist skilled in PENG block and caudal blocks will conduct the relevant block according to the group at 1 ml·kg−1 each utilizing a total of 0.25% ropivacaine with 1:200,000 epinephrine. They will not be involved in management of perioperative period and follow-up visit. Anesthesia is maintained with sevoflurane at a minimum alveolar concentration (MAC) level of 1.5 to keep that the bispectral index monitor (BIS) remains within the 40–60 range. Mechanical ventilation (6–8 ml·kg−1) with a 50% air/oxygen mixture is used; goal end-tidal carbon dioxide (ETCO2) pressure is maintained between 35 and 45 mmHg for both groups. An independent anesthesiologist who does not participate in regional anesthesia procedures manages hemodynamic parameters during surgery providing sufentanil and muscle relaxant drugs as needed by while keeping them within the preoperative baseline levels. A patient-controlled analgesia (PCA) pump will be activated 30 min prior to completion of surgery. The SLIPA removal will be thoroughly assessed by anesthesiologists immediately after surgery in the operating room.
Ultrasound-guided pericapsular nerve group blockThe patient is positioned supine with 90° abduction of the hip and knee, followed by adequate skin disinfection. The PENG block is performed using the ultrasound-guided technique described by Giron [11]. A 6–14 MHz linear transducer is placed in the transverse plane across the anterior inferior iliac spine (AIIS) and then rotated 30–45° to align with the pubic ramus [12]. AIIS, iliopubic eminence (IPE), iliopsoas tendon (IPT) are easily visible anatomical landmarks under ultrasound assistance. After positioning the ultrasound probe accurately, local anesthetic will be injected into the plane between IPE and IPT after negative aspiration utilizing an in-plane technique and a 22G*50 mm atraumatic needle for peripheral nerve blocks.
Caudal blockThe sacral hiatus can be detected using traditional anatomical landmarks in the left decubitus posture with flexed hips and knees. Firstly, by palpating the posterior superior iliac spines yields a line (known as Tuffier’s line) that forms the base of an equilateral triangle, with its tip identifying the position of the sacral hiatus [17]. A caudal needle is inserted at an approximate angle above the sacral hiatus under aseptic circumstances. Subsequently, changing to a flatter angle when the resistance is gone facilitates entrance into the epidural space. Above important, aspirating before injecting local anesthetic should be done with attention to avoid unintentional intravascular or spinal injection.
Ropivacaine concentrationThe venous blood samples will be taken at 10, 30, and 60 min after regional anesthesia. Following that, the plasma samples will be separated, frozen, and stored at − 80 °C until they can be analyzed within 1 h of collection. The amounts of ropivacaine will be measured by liquid chromatography tandem mass spectrometry [18].
Postoperative periodAll patients received standardized procedures from our hospital for post-trial care to ensure the safety of all patients. Following the removal of SLIPA, patients will be transported to the post-anesthesia care unit (PACU) for continued anesthesia recovery and achieving an Aldrete score ≥ 9. In all patients, a PCA pump containing sufentanil 2 μg·kg−1 and ondansetron 0.1 mg·kg−1 diluted in 100 ml of normal saline will be used for 72 h after surgery. The background infusion rate is set at 2 ml·h−1, with extra 0.5 ml boluses accessible upon patient request; however, each subsequent button press will be locked within a 15-min time period. If the PCA pump fails to provide adequate coverage (face, leg, activity, cry, consolability [FLACC] scores ≥ 4), a rescue analgesic consisting of intravenous sufentanil at a dose of 0.1 μg·kg−1 can be administered in the PACU or oral ibuprofen at a dose range between 5 and 10 mg·kg−1 can be given in the ward as an alternative measure, and all rescue analgesic will be recorded and analyzed. Using an electronic pain management database system, all data related to PCA pump usage, including the number and timing of button presses as well as drug consumption, will be accurately recorded in real-time.
OutcomesThe primary objective of this study is to compare the analgesic efficacy of ultrasound-guided PENG block to caudal block in pediatric patients with DDH who are scheduled for hip surgery.
Primary outcomeThe primary outcome of this study is the maximum FLACC score among the 5 time points (1 h, 3 h, 6 h, 12 h, and 24 h after extubation postoperatively).
Secondary outcomesThis study also assesses the following secondary outcomes:
(A)The total consumption of the opioids per weight intraoperative
(B)Consumption of analgesic medication (morphine equivalent) within 24 h postoperatively
(C)The timing of the first application of rescue analgesia
(D)Use of PCA pump (effective/ineffective pressing number)
(E)Time of SLIPA removal post-surgery
(F)The plasma concentration of ropivacaine
(G)Operation time for two blocks
(H)Possible related adverse events (urinary retention and vomiting, and block related)
(I)Hospital expenses and lengths of stay
Sample size calculationThe max FLACC scores at rest within 24 h postoperatively (1 h, 3 h, 6 h, 12 h, 24 h after extubation) are used as the primary outcome for sample size calculation in this study, which is planned as a non-inferiority trial, utilizing PASS software V.15.0.5. Based on our preliminary experimental data, where the maximum pain score postoperatively after caudal block was found to be 2.25 (0.38), assuming that PENG block reduces the pain score with a standard deviation 0.5 and setting a non-inferiority margin of 0.4, we will include a total of 42 participants (N1 = N2 = 21) and achieve an alpha level of set at 0.025 and power of 80%. With a 15% dropout rate, we estimate that the final sample size will be 48 participants (NI = N2 = 24).
Data collection and administrationEach participant’s case report forms (CRFs) will be completed, covering the preoperative, intraoperative, and postoperative periods. Prior to surgery, demographic information (sex, age, height, weight) and baseline characteristics (diagnosis, comorbidities, preoperative medications, allergy history, baseline MAP/HR values) will be gathered. Intraoperative and postoperative data, including vital signs monitoring, medication administration records, and FLACC scores, will be recorded. Withdrawals from the trial will be recorded in the CRFs as well. Two independent research assistants will input the CRFs data into an electronic case report file and double-check the information supplied. Unique numbers are used to distinguish patients in database after follow-up, instead of patient identity information, which is used in statistics analysis and publication. After that, all original data will be coded and safely kept in our archives.
Statistics analysisA statistician is in charge of data analysis with Statistical Product and Service Solutions (SPSS) Statistics for Windows, version 23.0. The analysis should consider all accessible data, with no exceptions for missing values. Patients with protocol non-adherence, such as those in the intention-to-treat group, will be reported in our research findings, for which intention-to-treat population analysis (ITT) and per-protocol analysis (PP) will be performed. When comparing two groups, normally distributed variables will be represented as mean (standard deviation, SD), while non-normally distributed variables will be provided as median [range]. Continuous variables will be given as mean (SD), whereas categorical variables will be reported as frequency or percentage. The T-test and rank-sum test will be used to compare measurement data between the two groups, while the χ2 test will be used to compare categorical data. The relative risk, as well as the 95% confidence interval (CI), will be determined. The pain score of the primary outcome will be compared between the two groups using repeated measure analysis of variance, with potential post hoc subgroup analyses undertaken if necessary. A significance level of P < 0.05 indicates statistically significant differences between the two groups.
Safety considerationRegional anesthesia will be provided in the operating room after general anesthesia, with continuous monitoring of vital signs. Any changes in vital signs will be noticed and addressed as soon as possible, and any unforeseen serious incidents related to this study will be reported to both the principal investigator and the hospital patient safety board. We have drawn up contingency plans such as local anesthetic poisoning include detailed therapeutic regimen. Medical costs related to all adverse events are free and the compensation to those who suffer harm will be discussed according to the relevant laws of China.
留言 (0)