
記住我


The intervention will be supervised by Physical Education professionals at all stages. It will consist of two arms, conducted in parallel, both with combined training differentiated by the environment (aquatic or dry-land).
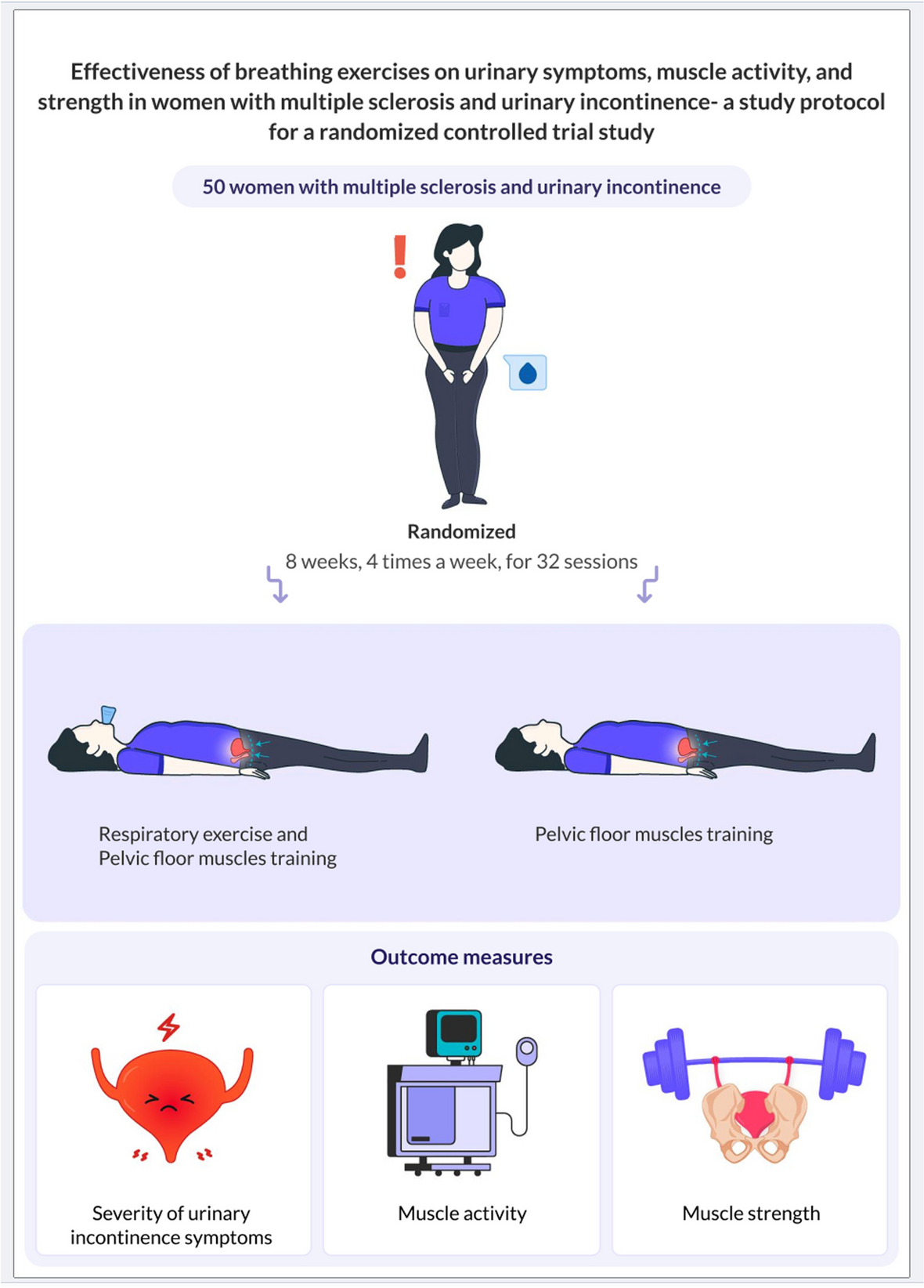
Intervention descriptionThe intervention period will take place during 24 weeks, with a frequency of three weekly sessions, on non-consecutive days (Monday, Wednesday, and Friday), with combined training carried out in an aquatic (swimming pool) or dry-land (athletic track) environment. Training sessions will last a maximum 60 min, distributed to 5 to 10 min warm-up, 30 to 50 min of main part (aerobic and resistance training), and 5 to 10 min of cool-down.
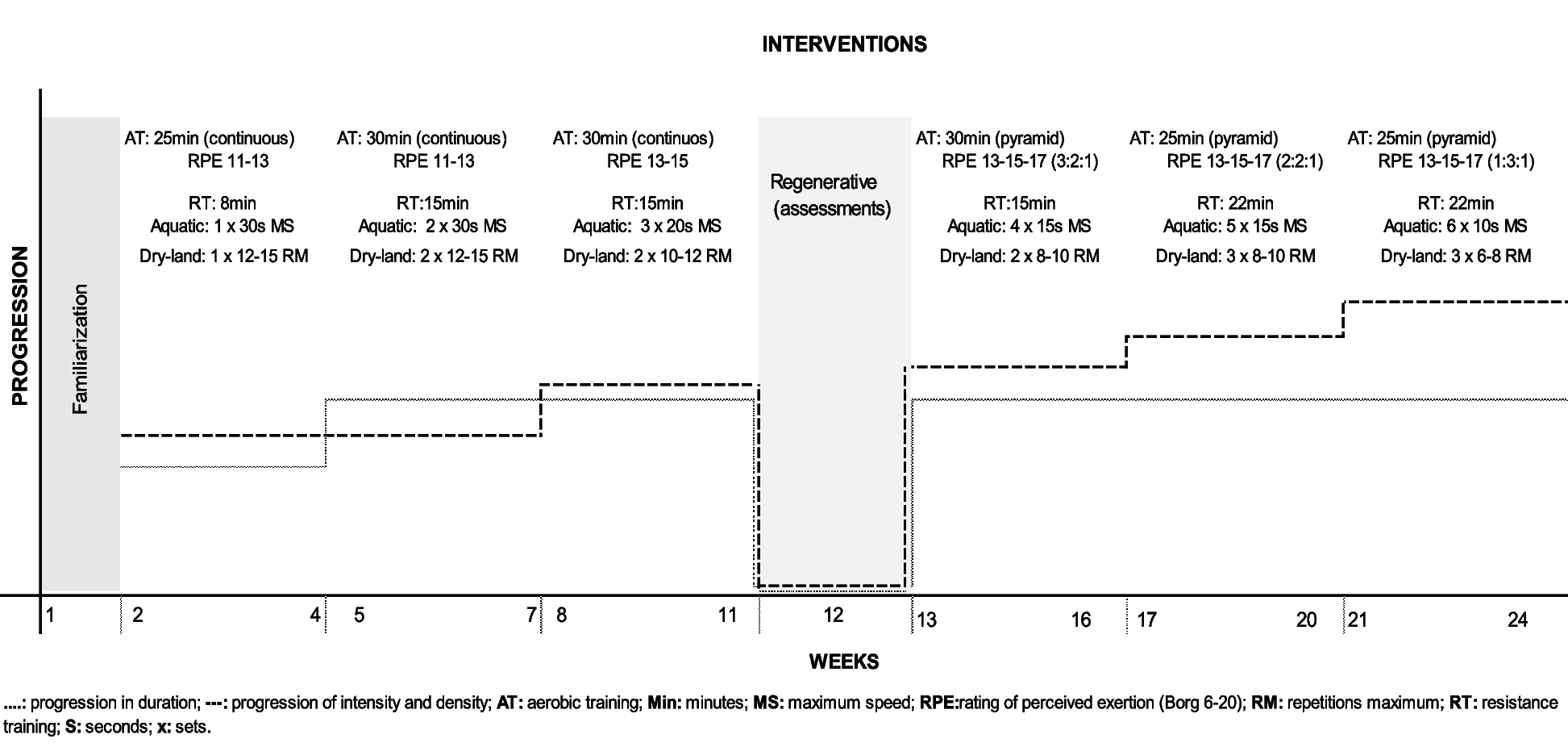
The 24 weeks of training for both groups will be divided into 6 mesocycles, starting with 1 week of familiarization. The first two mesocycles will each last 3 weeks, while the remaining mesocycles will each last 4 weeks. Aerobic aquatic and land training will be prescribed by a continuous method in the first 3 mesocycles, starting with 25 min in the RPE 11–13 intensity (Borg scale, 6 to 20 points), progressing in duration in the second mesocycle (30 min) and in intensity in the third mesocycle (RPE 13–15). In the following 3 mesocycles, it will be prescribed by the pyramidal method with intensity progression from light to strong (11 to 17) within blocks and with density progression along mesocycles. Resistance training will consist of exercises for the main muscle groups, using multiple sets, involving the resistance of water in the aquatic environment and the weight of equipment in the dry-land environment. The intensity of resistance training will be given by maximum speed (RPE 19) in aquatic environments and target repetition zone (15–6 repetitions) in dry-land environments (Fig. 1).
Fig. 1
Training program during the 24 weeks
Five lower limb exercises will be used for aerobic training in the aquatic environment: posterior stationary running, front kick, backward elevation, front slide, and stationary running, accompanied by upper limb movements (alternating front push, bottom-up dig, horizontal elbow flexion and extension, top-down dig, front cross push). Structuration will consist of two-block exercise, block 1 (horizontal shoulder flexion and extension crossing, unilateral hip flexion and extension with knee flexion and extension) and block 2 (horizontal shoulder flexion and extension crossing, unilateral knee flexion and extension), progressing from 1 set of 30 s until 6 sets of 10 s of execution in each exercise, with intervals of 1 min between sets and blocks and 10-s between exercises. Aerobic training on LAND will be carried out on a treadmill or athletic track land and will follow the same periodization as the group training in water. Resistance training on LAND will be prescribed by maximum repetition zones and will consist of 4 exercises (machine row, horizontal leg press, bench press, and knee flexion). This group will start with 1 set of 12 to 15 repetitions per exercise in the first mesocycle, increasing one set in the second mesocycle. The third mesocycle maintains the number of sets and increases the intensity with 10–12 repetitions per exercise, with progressions in intensity (8–10 repetitions) in the fourth mesocycle. In the fifth mesocycle, only the number of sets is increased to three and in the last mesocycle, only the intensity is modulated to 6–8 maximum repetitions. The interval between sets and exercises adopted was 1 min (Supplementary material).
There will be no modification to the participant’s allocation after allocation’ however, in severe cases of discomfort/injury, the protocol will be analyzed and adapted so as not to cause harm to the participants.
Safety and training monitoringAs monitoring and safety variables, information on internal and external load, capillary blood glucose, blood pressure, and affective response to exercise will be collected. The internal load will be collected using the adapted Borg Scale CR10 [40]. The external load in aerobic training in the aquatic training will be the number of knee elevations in the stationary running exercise, and in the resistance component, the volume will be by the number of movements in the knee extension and flexion exercise collected in all series. To quantify the external load in land-based aerobic training, the volume will be represented by the distance covered on the athletics track. With the duration and footage data, the speed will be calculated, representing the intensity of the aerobic component. In the resistance component, the volume will be represented by the number of repetitions (average between sets and/or total) in the leg press exercise, while the intensity will be represented by the weight used in this same exercise. External load assessment will be performed by capillary blood, collected with the Accu-Check® equipment (Roche, Portugal), and clinical blood pressure (BP), obtained using the OMRON automatic monitor (model HEM-7113, Brazil), before and immediately, 15 and 30 min after the first and last session of each training mesocycle.
To monitor the affective response to exercise, it will be applied the Sensation Scale of Hardy and Rejeski [41] in the first and last session of each training mesocycle.
Criteria for discontinuing or modifying allocated interventionsIntervention may be discontinued due to severe adverse events or patient requests.
Strategies to improve adherence to interventionsParticipants will be asked about the reasons related to adhesion, adherence, compliance, and withdrawal throughout the intervention. To understand the reasons for adhering to the intervention program, participants will be asked “What is the main reason that made you participate in this study?”. However, there were no strategies to increase adherence to the intervention.
Relevant concomitant care permitted or prohibited during the trialAll participants will be allocated to one of the two exercise interventions. Participants will be asked to refrain from extra exercise outside the research project.
Provisions for post-trial careAfter the conclusion of the clinical trial, participants will have access to ongoing care through supervised exercise programs conducted in both aquatic and dry-land environments. These programs will be offered through an extension project at UFSC, under the supervision of the project coordinator. They will be designed to support the participants' physical well-being, with strict monitoring to ensure safety and effectiveness. Furthermore, if significant changes are observed in the post-study examinations, participants will receive follow-up care from an endocrinologist to address any potential metabolic or hormonal alterations. These measures aim to provide continuous support and ensure the health and safety of participants after the study's completion.
OutcomesThe assessor of all outcomes will be blinded and performed by experienced researchers. The measures to characterize the participants will be collected in the pre-intervention period, through an anamnesis containing sociodemographic information (sex, age, education, and marital status) and health (comorbidities, history of injuries and/or surgeries, use of medications with the quantity and dosages of medications). Nutritional assessment, level of physical activity, and sedentary behavior will be measured before and after 24 weeks of intervention.
Glycemic profile, lipid profile, plasma renin activity, C-reactive protein, neuromuscular and cardiovascular parameters, functional capacity, mental and cognitive health, sleep quality, and quality of life will be assessed at baseline, at the 12th and after 24 weeks of intervention. The other outcomes will be assessed before and after 24 weeks.
Features measures Nutrition monitoringNutritional monitoring will take place with the application of the “How is your diet?” test, developed by the Brazilian Health Ministry [42], which evaluates the portions of the group of fruits, vegetables, cereals, meat, legumes, milk, and foods rich in fats and sugars; type of fat used for cooking; and consumption of saturated fat, cholesterol, and added salt. Furthermore, it seeks to identify the number of meals and intake of water and alcoholic beverages.
Physical activity levels and sedentary behaviorThe level of physical activity and sedentary behavior will be measured using triaxial accelerometer model wGT3X-BT (ActiGraph LLC, Pensacola, FL, USA) on the non-dominant wrist. For this verification, participants will be instructed to use the accelerometer for 24 h (except for activities in which the monitors are submerged in water) for 7 days of the week. For physical activity level analysis, data will be processed using the “GGIR” package, version 2.0.2, in R (R Foundation for Computing Statistics, Vienna, Austria). Data will be valid and included in the analyses when the monitor is used for at least 16 h on four or more weekdays and at least one weekend day) [43].
A sampling rate of 30 Hz will be used to collect data, and it will be analyzed in 5-s intervals (epochs) to measure physical activity levels. Physical activity will be quantified in milligravity units (mg) and categorized into sedentary behaviors (≤ 18 mg), light physical activity (18 mg to 59 mg), and moderate physical activity (≥ 60 mg) [44]. The duration of the sedentary behavior and physical activity sessions will be evaluated based on the criteria of continuous sessions, sessions of 10, 20, 30, and 60 min for sedentary behavior and light physical activity, and sessions of 1.5 and 10 min for moderate physical activity.
Primary outcomeThe primary outcome will be the levels of glycated hemoglobin (HbA1c), which will be assessed from a sample of total blood using the high-performance liquid chromatography (HPLC) methodology on automated equipment.
Secondary outcomesAs secondary outcomes, biochemical markers, functional capacity, anthropometrics and body composition, cardiovascular, neuromuscular parameters, and behavioral and psychosocial parameters will be evaluated.
Biochemical markersBlood collection will be by venipuncture at the Sabin Laboratory by a nursing professional or nursing technician experienced in the procedure, following standardized protocols. Patients will be instructed to maintain their usual dietary pattern (collection in a fed state) or fasting for at least 8 or 12 h before the blood sampling.
From the collected blood, a hemogram will be carried out in order to evaluate the participants’ red blood cells, leukocytes, and platelets, and serum lipids (total cholesterol, HDL, and triglycerides), glucose, creatinine, and insulin will also be measured, all on the BS 120 Mindray® automation equipment using the available reagent kit, following the manufacturer’s instructions. Insulin resistance will be estimated using the homeostasis model assessment of insulin resistance (HOMA-IR) [45]. LDL cholesterol will be calculated using the Friedewald formula [46]. Plasma renin activity will be analyzed from serum using the enzyme-linked immunosorbent assay (ELISA) method, following the instructions of the manufacturer (BD Biosciences Pharmingen, San Diego, CA), with a detection limit of 2.2 pg/mL. The C-reactive protein (CRP), a pro-inflammatory marker, also will be analyzed.
Subsamples of brain-derived neurotrophic factor (BDNF) and irisin also will be evaluated by enzyme-linked immunosorbent assay (ELISA) method in a laboratory of the Federal University of Santa Catarina.
Functional capacityTo assess functional capacity, flexibility, lower limb strength, endurance, and functional mobility tests will be carried out. The “sit and reach” test will be performed to assess lower limb flexibility using the Wells bench [47]. Lower limb muscle strength and endurance will be evaluated through the 30-s sit-stand test according to the Rikli and Jones protocol [48]. Based on data from the sit-stand test, the muscular power of the lower limbs will be calculated using the equation by Alcazar et al. [49], described as follows: MP = 0.9 × [participant height × 0.5 − chair seat height]/number of repetitions in the sit-stand test × 0.1. To assess functional mobility, the Timed Up-and-Go (TUG) test will be performed at two speeds, (1) maximum (TUG-m) and (2) usual (TUG-h) [50]. To evaluate the interference of the dual task on the participant’s performance in the TUG test, two adaptations of the test will be carried out, the animal TUG (TUG-a) and the previous month’s TUG (TUG-pm) [51]. To assess functional cardiorespiratory fitness, the 6-min walk test (6MWT) will be performed [52].
Maximum strength and muscle endurance of knee extensorsThe one-repetition maximum (1RM) test will be performed for the lower limbs in the knee extension exercise. Previously to the assessment, the patients will warm up during the exercise itself, performing 1 set of 20 repetitions with a very light load. Subsequently, a load will be selected so that the subjects perform a maximum of 10RM. After the participants perform the maximum number of repetitions, the load will be adjusted in order to find the 1RM, according to Lombardi coefficients [53], until the maximum load is found. A maximum of five attempts will be made, with a 5-min break between each attempt. The execution speed adopted will be 1.5 s for the concentric phase and 1.5 s for the eccentric phase, controlled by a metronome. To determine the resistance strength, the number of repetitions performed with 60% of 1RM will be considered, following a pre-established cadence and amplitude of execution. In the post-training evaluation, the load corresponding to 60% of the 1RM test carried out in pre-training will be used. Two days of familiarization with the 1RM test will be adopted, with 2 sets of 10–15 submaximal repetitions at the test cadence and standardized amplitude.
Body composition and anthropometricsMeasurements of body composition and anthropometry will be taken together, in the same order and in the morning with at least 8 h of fasting. All participants will be instructed not to practice physical exercise the day before data collection and to abstain from alcoholic, caffeinated, and other diuretic drinks in the 48 h prior to the test and not having a menstrual period in the case of women. Participants will also be wearing clothes without zippers or metal, will be without earrings or rings or any other type of metal, and will urinate 30 min before the assessment.
Computed densitometry by dual-energy radiological absorptiometry (DXA) Hologic®, model Discovery WI Fan-beam—S/N 81593 (Hologic, Inc., Bedford, MA, USA) will be used to assess body composition. The device will be calibrated before the analyses and will be used following the manufacturer’s recommendations. The assessment will be done in automatic and whole-body mode. Bone mineral density, lean mass, fat mass, adipose, and lean indices that are delivered by the analysis will be used.
Bioimpedance (BIA), multifrequency InBody® 720 model (Biospace, Los Angeles, USA), with eight electrodes, measuring resistance at five frequencies (1, 50, 250, 500, and 1000 kHz) and reactance in three (5, 50, and 250 kHz) will be used to estimate raw values of resistance (R) and reactance (Xc) which will be used to estimate the phase angle (PhA). The technique provides impedance (Z) and Xc data at a frequency of 50 kHz, and from these, the R value will be calculated by the proportional sum of the body, in which the upper limbs represent 40% of the total body, the torso represents 10%, and the lower limbs represent 50%. In this way, the PhA, expressed in degrees, will be calculated using the equation PhA = Arctangent (Xc/R)*(180/π) [54]. The device will be calibrated and used in accordance with the manufacturer’s recommendations. Body mass will be measured using the previously mentioned BIA device and height (stadiometer, Alturaexata®, with 1 mm precision) will be measured with the participant remaining at maximum inspiration, on their back, and with the rod positioned over the head. Both data will be used to determine the body mass index (BMI) using the formula body mass (kg)/height (m2). Waist, abdominal, and calf circumferences will be obtained using the procedures described by Lohman, Roche, and Martorell [55] with a Cescorf® brand measuring tape, with a precision of 0.1 cm. Subsequently, the waist-to-height ratio (WHtR) will be calculated using the formula waist circumference (cm)/height (cm). Both protocols will be applied by experienced researchers trained in using the device.
Cardiovascular measuresClinical blood pressure (BP) measurements will be obtained using the OMRON automatic monitor (model HEM-7113, Brazil), following the recommendations of Brazilian Guidelines for In-office and Out-of-office Blood Pressure Measurement [56], on two non-consecutive days. On each day, the participants will remain at rest, lying, in a calm environment, for 10 min, and three measurements will be taken, with a 1-min interval, on the left arm, using the average of the last two measurements. If there is a difference of > 10 mmHg between these last two measurements, additional measurements will be taken. Mean arterial pressure (MAP) will be calculated using the following formula: MAP = (SBP − DBP)/3 + DBP.
The autonomic modulation of the cardiovascular system will be assessed using the heart rate variability technique. For this, after 10 min of resting, the subjects will remain lying down for 10 min, during which time the RR intervals will be recorded using a heart rate monitor valid for this function (Polar V800, Polar Electro, Finland). Afterwards, at least 5 min of the stationary signal will be considered for analysis as a valid signal, which will be evaluated by an experienced researcher. After collection, the RR intervals will be exported to the Kubios HRV program (Biosignal Analysis and Medical Imaging Group, Finland), whose analyses will be performed (time and frequency domain). The time domain parameters, standard deviation of all RR intervals, square root of the mean of the square of differences between adjacent normal RR intervals, and percentage of adjacent intervals longer than 50 ms will be obtained [57]. The frequency domain parameters will be obtained by the spectral analysis technique, using the autoregressive method, with the model order set at 12. Frequencies between 0.04 and 0.4 Hz will be considered as physiologically significant, with the low component being frequency (LF) represented by oscillations between 0.04 and 0.15 Hz and the high-frequency component (HF) between 0.15 and 0.4 Hz. The power of each spectral component will be calculated in normalized terms, dividing the power of each band by the total power, from which the value of the very low-frequency band (< 0.04 Hz) will be subtracted, and the result will be multiplied by 100. The sympathy-vagal balance will be determined by dividing LF by HF, given that the LF and HF bands are considered sympathetic and parasympathetic modulation parameters, respectively [57].
Vascular function will be assessed using the flow-mediated dilation (FMD) technique, following current recommendations [58], using the LOGIQ S7 Expert Ultrasound device (GE Healthcare). Subjects will receive the following recommendations, previously: (a) fast for at least 6 h, (b) avoid exercise for at least 24 h, (c) avoid alcohol and foods or drinks that contain caffeine or are rich in polyphenols for at least 12 h; (d) do not smoke or consume tobacco for at least 6 h. Initially, individuals will lie supine, for 10 min, in a silent environment and preferably in the dark. After this moment of rest, an initial resting BP measurement will be taken, with the cuff located on the left arm. Blood flow velocity spectra will be recorded simultaneously through pulsatile mode at a linear frequency of 10 MHz with an inclination angle of 60°. Diameter and baseline blood flow will be recorded continuously over 90 s. After baseline recording, a cuff positioned on the forearm will be inflated, which will have a pressure 50 mmHg above the systolic blood pressure, measured prior to the exam. The occlusion will be maintained for 5 min and, after this period, quickly released. Doppler recordings will resume 30 s before cuff deflation and will be maintained for an additional 180 s. Post-occlusion diameter and blood flow will be measured after release. Vasodilatory capacity will be calculated as the percentage increase in post-occlusion artery diameter in relation to baseline values. All images will be transferred using video capture software (OBS Studio, 26.0.2) at a frequency of 30 Hz and saved on an external hard drive for later analysis using semi-automatic software (Cardiovascular suite 4—FMD Studio software, Institute of Clinical Physiology, Italy). The baseline diameter will be defined as the average of 90 s of data obtained before cuff inflation. The peak diameter will be defined as the largest diameter value found after releasing the cuff. Vasodilation mediated by radial and brachial artery flow will be calculated as the percentage difference between the basal diameter and the peak diameter. The data will be presented by the software as anterograde shear rate (SRANT) and retrograde shear rate (SRRET). The mean shear rate (SRMEAN) will be calculated as the difference between the anterograde and retrograde components. The area under the shear rate curve (AUCSR), indicative of the stimulus for vasodilation, will be calculated from the moment of cuff release until the peak diameter is reached. Blood flow will be calculated using the formula “Flow = Vmπ(D2/4) × 60,” in which Vm corresponds to the average speed of blood flow in centimeters per second and D represents the diameter of the brachial artery in centimeters. The average speed will be obtained by the formula “Vm = (SRMEAN × D)/4.” The flow oscillation index will be determined as “SRRET/(SRANT + SRRET),” with the values obtained ranging from 0 to 0.5 indicating unidirectional laminar flow and pure oscillation, respectively [58].
Mental and cognitive health, sleep quality, and quality of lifeTo assess depressive symptoms, the PHQ-9 questionnaire will be used, which consists of nine items, including symptoms and attitudes, whose intensity varies from zero to three, with 27 being the maximum score [59]. To track the participants’ cognitive status and classify them regarding the presence of mild cognitive deficits or dementia, the MoCA instrument [60] translated into Portuguese [61] and validated for the Brazilian population [62] will be used. Furthermore, to verify specific domains of cognitive function, working memory will be assessed using the Digit Span, inhibitory control using the Stroop Color Test, and cognitive flexibility using the alternating verbal fluency test [63, 64]. Sleep quality will be assessed using the Pittsburgh scale [65, 66]. To assess quality of life, the WHOQOL-8 instrument [67] will be used. The patients’ perspective regarding the impact of diabetes and treatment on their lives will be assessed using the Problems Areas in Diabetes Scale (PAID) questionnaire translated and validated into Portuguese [68].
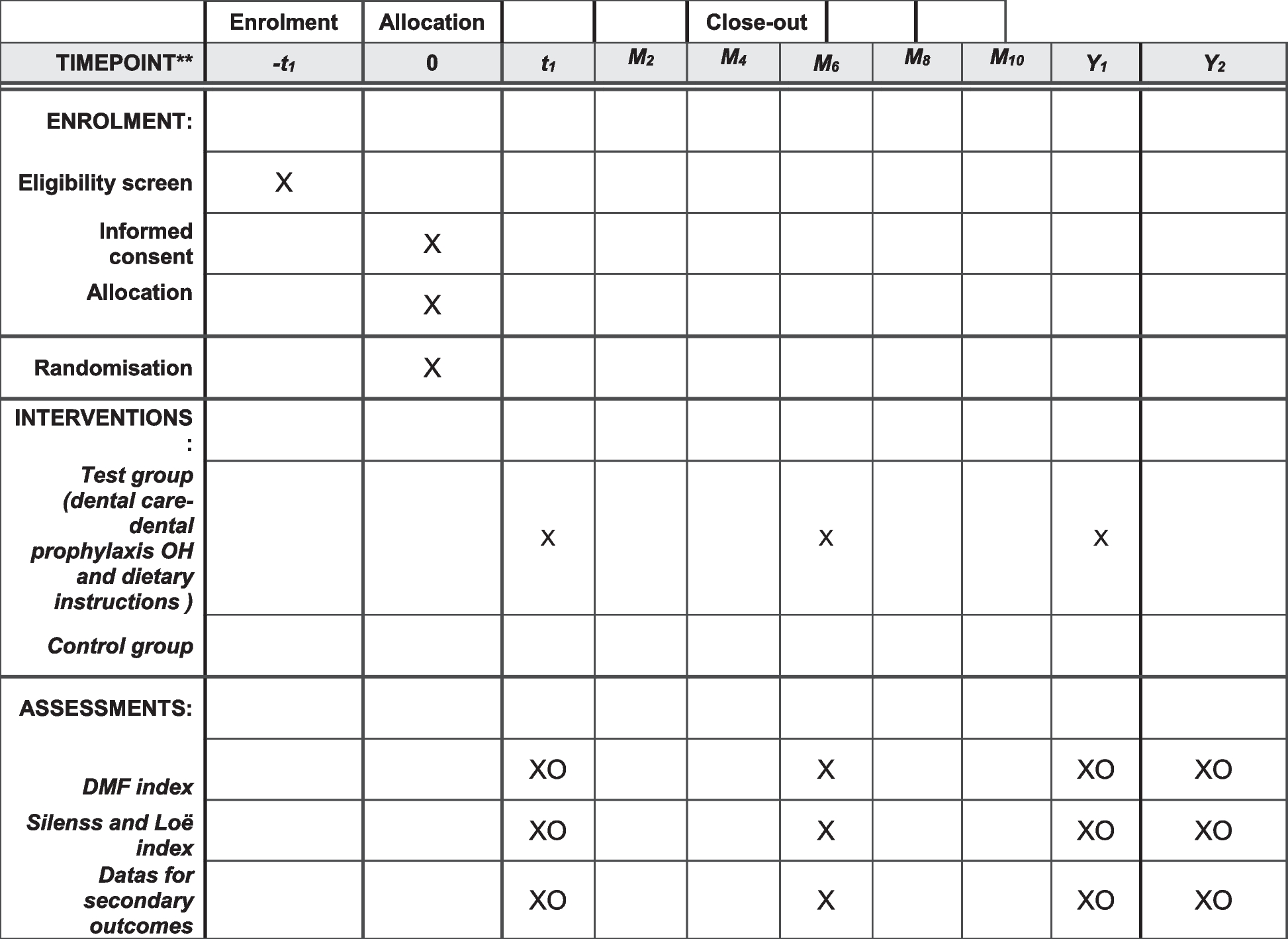
Participant timelineParticipant timeline and checkpoints are summarized in Fig. 2.
Fig. 2
Standard Protocol Items: Recommendations for Interventional Trials SPIRIT Figure. Note: BP= blood pressure; HDL-C= High-Density Lipoprotein Cholesterol; HOMA-IR= Homeostasis Model Assessment of Insulin Resistance; HR= heart rate; LDL-C= Low-Density Lipoprotein Cholesterol; TC= total cholesterol; BDNF= Brain-Derived Neurotrophic Factor
Sample sizeThe sample size calculation was carried out based on 5% of significance, a power of 80%, an effect size f of (0.129), corresponding to a difference of – 0.4% in HbA1c for AQUA compared to LAND, and a 1:1 relationship between groups. Thus, the calculation demonstrated the need for a minimum of 25 participants in each group. Considering a sample loss similar to that found in the study by Delevatti et al. [69], which was 30%, a sample size of 32 participants in each group (64 participants involved in the study) will be recruited. G-Power 3.1.6 program (University of Dusseldorf, Düsseldorf, Germany) was used for the analysis.
RecruitmentThe recruitment began in April of 2024. A dissemination strategy will be organized via social networks (email lists, Instagram®, websites), posters at UFSC, delivery of flyers nearby, and via advertisements on radio, newspapers, and television programs. From the initial contact of interested through telephone calls, emails, or face-to-face, this information will be stored in a database that will be used to contact participants who meet the requirements for the interview. To this end, participants will be invited to attend the university on a scheduled date and time to fill out an anamnesis focusing on lifestyle and health characteristics to confirm eligibility and clarify the objectives and procedures of the research and, if they accept, they will sign a consent form and the initial assessment battery will be scheduled.
留言 (0)