
記住我
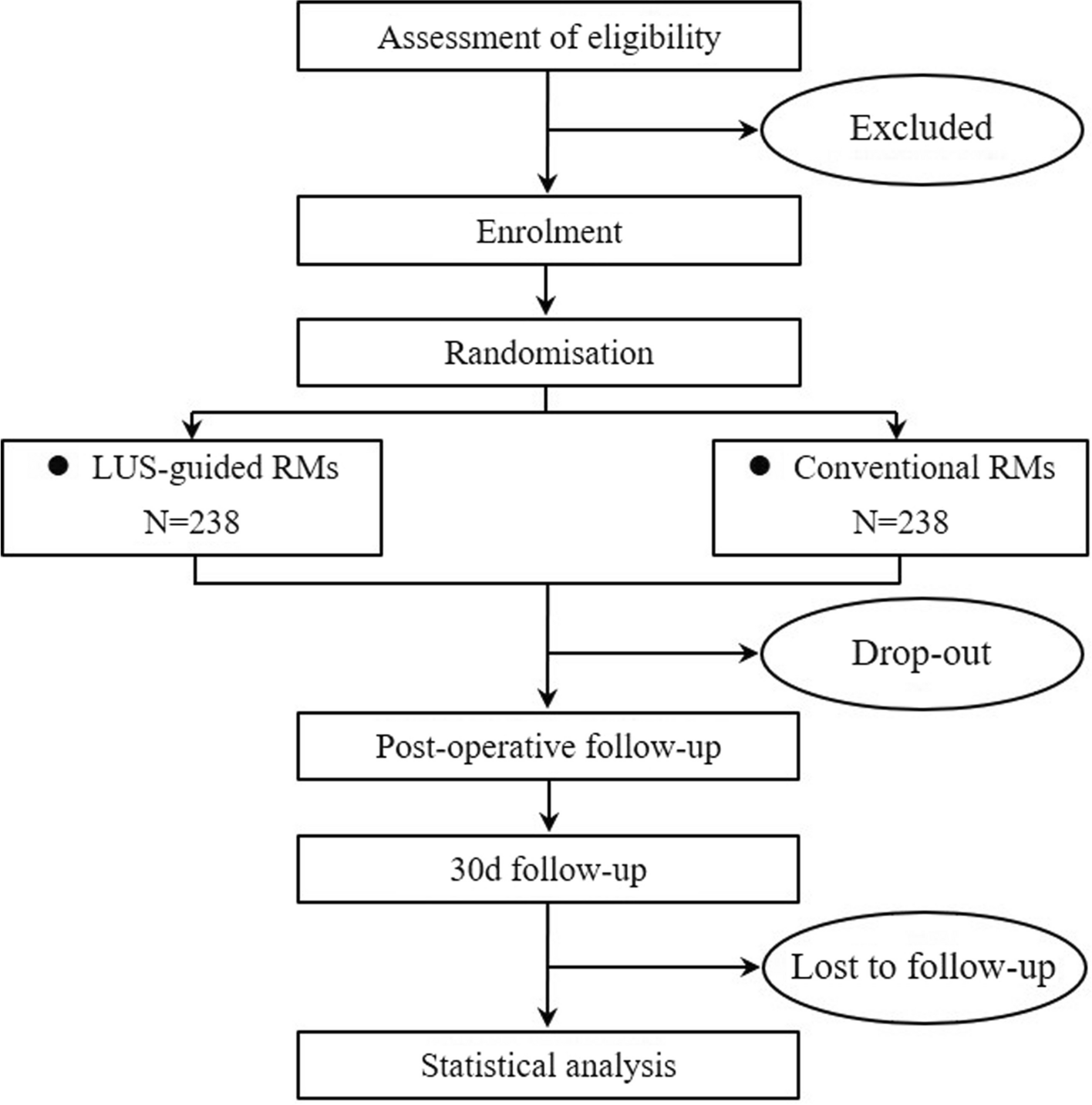


This prospective, randomised, two-arm clinical trial will test the hypothesis that RMs conducted with the guidance of LUS, compared with conventional RMs, reduce the incidence of PPCs in obese patients scheduled for laparoscopic bariatric surgeries. In total, 476 patients from the Third People’s Hospital of Chengdu will be randomly assigned to one of two different intraoperative RMs strategies (see the Consolidated Standards of Reporting Trials [CONSORT] diagram, Fig. 1). A complete checklist of recommended items to address in a clinical trial protocol and related documents according to the “Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2013” is provided in Additional file 1.
Fig. 1
Consolidated Standards of Reporting Trials (CONSORT) diagram. LUS, lung ultrasound; RMs, recruitment manoeuvres
This trial will be conducted following the WMA of the Declaration of Helsinki and the CIOMS Principles of the International Guidelines for Biomedical Research Involving Human Subjects. This study was approved by the Ethics Committee of the Third People’s Hospital of Chengdu on 27 December 2023 (approval number: S-237, 2023) and registered in the Chinese Clinical Trial Registry (ChiCTR) on 23 January 2024 (registration number: ChiCTR2400080203). Any deviation from the protocol will be fully documented using a breach report form. What is more, ethical committee’s approval will be required again. We will also update the protocol in the ChiCTR website.
Study populationInvestigators will screen and recruit obese patients scheduled for laparoscopic metabolic and bariatric surgery in the ward the day before surgery. The inclusion criteria are listed as follows: aged older than 18 years, American Society of Anaesthesiologists (ASA) physical status I–III, meeting the criteria for surgical indications specified in the Chinese guidelines for bariatric surgery [24] and provided informed consent. The exclusion criteria are listed as follows: already participated in another trial, the existence of severe chronic obstructive pulmonary disease (COPD, defined as GOLD grades III–IV) and a history of severe or uncontrolled bronchial asthma, cardiac dysfunction (defined as New York Heart Association class III or IV), ongoing renal replacement therapy before surgery, intracranial injury, or tumour, or neuromuscular disease and expected to require prolonged postoperative mechanical ventilation (due to difficult airway or planned administration in the intensive care unit (ICU)).
InterventionRMs will be performed immediately after successful endotracheal intubation and at the end of the surgery. The intervention group underwent real-time LUS-guided RMs (group L): manual re-expansion with a gradual increase in airway pressure until no atelectasis was observed in the lung images, with a maximum airway pressure limit of 45 cmH2O, and a tidal volume not exceeding 20 ml/kg of adjusted body weight (ABW) [ABW = ideal body weight (IBW) + (0.4 * (total body weight (TBW) − IBW), male IBW = height (cm) − 100, female IBW = height (cm) − 105]. The control group underwent conventional manual RMs (group C): manual squeezing of the bag to a peak pressure of 40 cmH2O, maintained for 10 s. The systolic blood pressure should not be lower than 90 mmHg or the heart rate lower than 50 bpm during RMs. When deemed intolerance of the RMs by the attending anaesthesiologists, rapid infusion of fluids and administration of vasoactive drugs are employed to ensure haemodynamic stability.
Perioperative lung ultrasound examinationThe RMs guided by intraoperative LUS are performed by anaesthesia care providers who have received standardised training in LUS and have conducted more than 100 practical cases. They are not involved in other tasks of this study, such as assessment of indicators and follow-up. LUS examinations are independently performed before induction and 30 min after endotracheal extubation by two experienced investigators blinded to the group assignment, using a SONIMAGE HS1 Ultrasound System (Konica Minolta Medical Technology (Shanghai) Co., LTD) with a C5-2 convex array probe of 2–5 MHz. All the participants are scanned in a semi-Fowler’s position in the post-anaesthesia care unit (PACU). Each hemithorax is divided into six quadrants by the anterior axillary line, the posterior axillary line and the horizontal line beneath the nipple [13]. The video clip of the most pathological areas of the intercostal space in each region is captured for analysis and scoring. Moreover, each of the 12 regions is assigned a score of 0–3 based on the following scoring system: 0, 0–2 B lines; 1, at least 3 B lines or small subpleural consolidations separated by a normal pleural line; 2, multiple coalescent B lines or multiple small subpleural consolidation separated by a thickened or irregular pleural line; and 3, consolidation or subpleural consolidation of more than 1 cm × 2 cm. The LUS (0–36) is calculated by summing the scores of all the 12 regions, with higher scores indicating more severe aeration loss [13].
Blinding, randomisationThis is a patient- and evaluator-blinded trial. The patients and their family members are not informed of the group assignments. Additionally, the surgeon and nurses in the surgical ward, the data collectors, the follow-up personnel and the statistical analysts are all unaware of the group assignments.
The eligible participants will be randomly allocated at a 1:1 ratio to group L or group C. They will be informed of the study details and provided with preoperative education to enhance compliance and cooperation. Informed consent will be obtained by a resident the day before surgery. The randomised sequence table correlating serial numbers, random numbers and group numbers was generated by SPSS 26.0 (IBM, Chicago, IL, USA) by an independent researcher not involved in other tasks of this study. The anaesthesia care providers open the opaque envelope before induction and perform the intraoperative RMs according to the predetermined group assignment. Therefore, all the attending anaesthesiologists are unblinded but not involved in the other tasks of the trial. In the circumstances where severe complications occurred during RMs, such as pneumothorax, the emergency unblinding are permitted.
Perioperative managementRoutine monitoring, which included a three-lead electrocardiogram, peripheral oxygen saturation (SpO2), non-invasive blood pressure measurement and bispectral index, is initiated once the patient entered the operating room. The usual care pathway will not be altered in both trial arms. An intravenous access for fluid administration is established for routine induction of general anaesthesia by attending anaesthesiologists. The medication and other advanced monitoring technics are determined at their own discretion. Flurbiprofen axidate 40 mg is administered prior to the operation. Nausea and vomiting prevention are achieved by administering dexamethasone 8 mg after the induction of anaesthesia and ondansetron 8 mg at the end of the surgery. Endotracheal intubation is performed by using a video laryngoscope after 5 min of mask ventilation with an 80% fraction of inspired oxygen (FiO2) at a fresh flow of 8 L/min. Anaesthesia is maintained by intravenous infusion of sevoflurane and continuous remifentanil to achieve a bispectral index between 40 and 60. Neuromuscular blocking is maintained intermittently with cisatracurium, which is monitored by train-of-four or by the requirement of the surgeon. The mean arterial pressure is maintained at 65–100 mmHg, and the heart rate is maintained at 50–100 bpm. The FiO2 is initially set at 40% with a fresh flow of 2 L/min to maintain the SpO2 greater than 94%. Once SpO2 < 94% develops, the rescue RMs will be applied after excluding the increased airway pressure caused by excretion and ventilator malfunction. In any rescue situation, the anaesthesia care provider could increase FiO2 if SpO2 deteriorates further. The pneumoperitoneum is standardised in our centre by applying 14 cmH2O of abdominal pressure. At the end of surgery, the administration of sevoflurane and remifentanil are discontinued. The fresh gas flow is increased to 8 L/min of oxygen, whilst the FiO2 is still set at 40%. Neuromuscular block is antagonised using prostigmine and atropine if necessary. Additionally, a self-controlled intravenous analgesia pump is provided for postoperative pain relief.
Mechanical ventilationAfter tracheal intubation with a reinforced, cuffed endotracheal tube with an internal diameter of 7.0 mm for female patients and 7.5 mm for male patients, lung protective ventilation is performed for all the participants with a tidal volume of 6–8 ml/kg (ABW) using volume control ventilation. The initial respiratory rate is 12 bpm, and then it is adjusted to maintain the partial pressure of end-tidal carbon dioxide between 35 and 45 mmHg. The inspiration to expiration ratio is set to 1:2. The peak inspiratory airway pressure limit is 45 mmHg. The setting of positive end-expiratory pressure (PEEP) is left to the independent anaesthesiologists in charge of surgery autonomously.
All the patients are extubated with positive airway pressure in the operating room and then transferred to the PACU in a semi-Fowler’s position, breathing the room air. Nasal oxygen supply is given to achieve an oxygen saturation of at least 94%. For patients with sleep apnoea syndrome, they also received their personal continuous positive airway pressure (CPAP) in the recovery room or the ward if deemed necessary by the doctors. Patients will be discharged from the PACU assessed by the modified Aldrete score standard.
Study outcomesThe primary outcome is the incidence of a collapsed composite of all PPCs developing within the first 5 postoperative days. With this approach, each weighted equally. Participants who developed at least one complication are considered as meeting the primary outcome.
The PPCs are defined as follows [25, 26]:
1.Pneumonia (using to the US Centres for Disease Control Criteria [27]);
2.Respiratory failure (according to the Berlin Definition [28]);
3.Bronchospasm (newly detected expiratory wheezing treated with bronchodilators);
4.Pleural effusion (chest X-ray demonstrating blunting of the costophrenic angle, loss of the sharp silhouette of the ipsilateral hemidiaphragm in upright position, evidence of displacement of adjacent anatomical structures, or [in supine position] a hazy opacity in one hemithorax with preserved vascular shadows, needing thoracentesis);
5.Pneumothorax (air in the pleural space with no vascular bed surrounding the visceral pleura, resulting in closed thoracic drainage);
6.Atelectasis (lung opacification with a shift of the mediastinum, hilum, or hemidiaphragm toward the affected area, as well as compensatory overinflation in the adjacent non-atelectatic lung detected via computed tomography or chest radiography);
7.Pulmonary aspiration (clear clinical history AND radiological evidence); and
8.Cardiogenic pulmonary oedema (clinical signs of congestion, including dyspnoea, oedema, rales, and jugular venous distention, with chest X-ray demonstrating an increase in vascular markings and diffuse alveolar interstitial infiltrates).
The secondary clinical outcomes are as follows:
1.The LUS score at 30 min after endotracheal extubation in the PACU.
2.The severity of PPCs [25]:
(i)None: planned use of supplemental oxygen or mechanical respiratory support as part of routine care, but not in response to a complication or deteriorating physiology. Therapies that are purely preventive or prophylactic, for example, high-flow nasal oxygen or CPAP, should be recorded as none;
(ii)Mild: therapeutic supplemental oxygen < 0.6 FiO2.
(iii)Moderate: therapeutic supplemental oxygen ≥ 0.6 FiO2, requirement for high-flow nasal oxygen, or both.
(iv)Severe: unplanned non-invasive mechanical ventilation, CPAP or invasive mechanical ventilation requiring tracheal intubation.
3.Intraoperative and postoperative safety-related events included hypoxemia (defined as SpO2 < 94%), hypotension (defined as systolic blood pressure < 90 mmHg) and bradycardia (defined as heart rate < 50 bpm).
4.The emergency time (from the withdrawal of general anaesthetics to endotracheal extubation) and the length of postoperative hospital stay.
5.Unexpected need for ICU admission.
6.The quality of postoperative recovery at 30 days after discharge (according to the QoR-15 score [29]).
Sample size calculation and statistical analysisThe sample size calculation of this trial is based on the primary outcome, the incidence of PPCs, which was reported to be approximately 24% according to a recently published international study in obese patients [30]. We assumed that LUS-guided RMs would reduce the incidence of PPCs by 50%, with a probability of α = 0.05 to allow for type 1 error and a power of 80%. Then, 226 subjects are needed in each group by using the PASS 15.0 software. A final sample size of 238 per group accounted for a 10% dropout rate in case follow-up (a total of 476).
After the trial is completed, the research team will work with medical statisticians to analyse the data. SPSS 26.0 statistical software is used for analysis, and GraphPad Prism 8.0 is carried out for graphics production, following the principle of intention-to-treat (ITT) analysis. The outcomes will be analysed as randomised, regardless of protocol adherence. All statistical tests are conducted by two-sided test, and differences will be considered statistically significant if P < 0.05. If missingness is > 5% for any variable, the mean normal value of the patient group will be used for imputation. The normality and variance homogeneity of the data will be assessed by using the Kolmogorov–Smirnov and Levene’s tests. Normally distributed data are presented as the mean and standard deviation (SD) and are analysed with Student’s t-test. For non-normally distributed data, median (quartile range) will be represented, and the Mann–Whitney U test will be applied. Categorical data will be presented as number (percentage). The difference in proportions will be evaluated using chi-square or Fisher’s exact test and the risk ratio of the associated 95% confidence interval (CI). The continuous data are compared using the one-way analysis of variance or the non-parametric Kruskal–Wallis test. Subgroup analysis is conducted based on potential risk factors affecting the occurrence of PPCs in bariatric surgery patients, including gender, age over 40 years, smoking status, body mass index (BMI) > 40, cardiopulmonary exercise test (CPET) grade and preoperative pulse oxygen saturation (with a threshold of 96%).
Data collection and recordingThe preoperative demographic parameters included gender, age, height, present weight, ideal weight, BMI, smoking habits, difficult airway assessment, ASA grade, smoking history and alcohol consumption history. Pre-existing comorbidities included diabetes mellitus or impaired glucose tolerance, hypertension, polycystic ovary syndrome, sleep apnoea syndrome, chronic obstructive pulmonary disease and asthma. A history of previous or current diagnosis of depression will also be recorded. Additionally, all patients underwent a CPET 1 week before surgery to evaluate their fundamental cardiopulmonary capacity.
Intraoperative parameters included pulse oxygen saturation, lung compliance, PEEP, fluid infusion volume, blood product transfusion, muscle relaxant drug dose and operation time.
Postoperative parameters included length of hospital stay, any cardiopulmonary complications and adverse events. In addition to preoperative visits, participants are also visited daily from postoperative day 1 to 5 as well as contacted by phone at 30 days after discharge. At different stages, patients’ data are collected and recorded on a case report form (CRF).
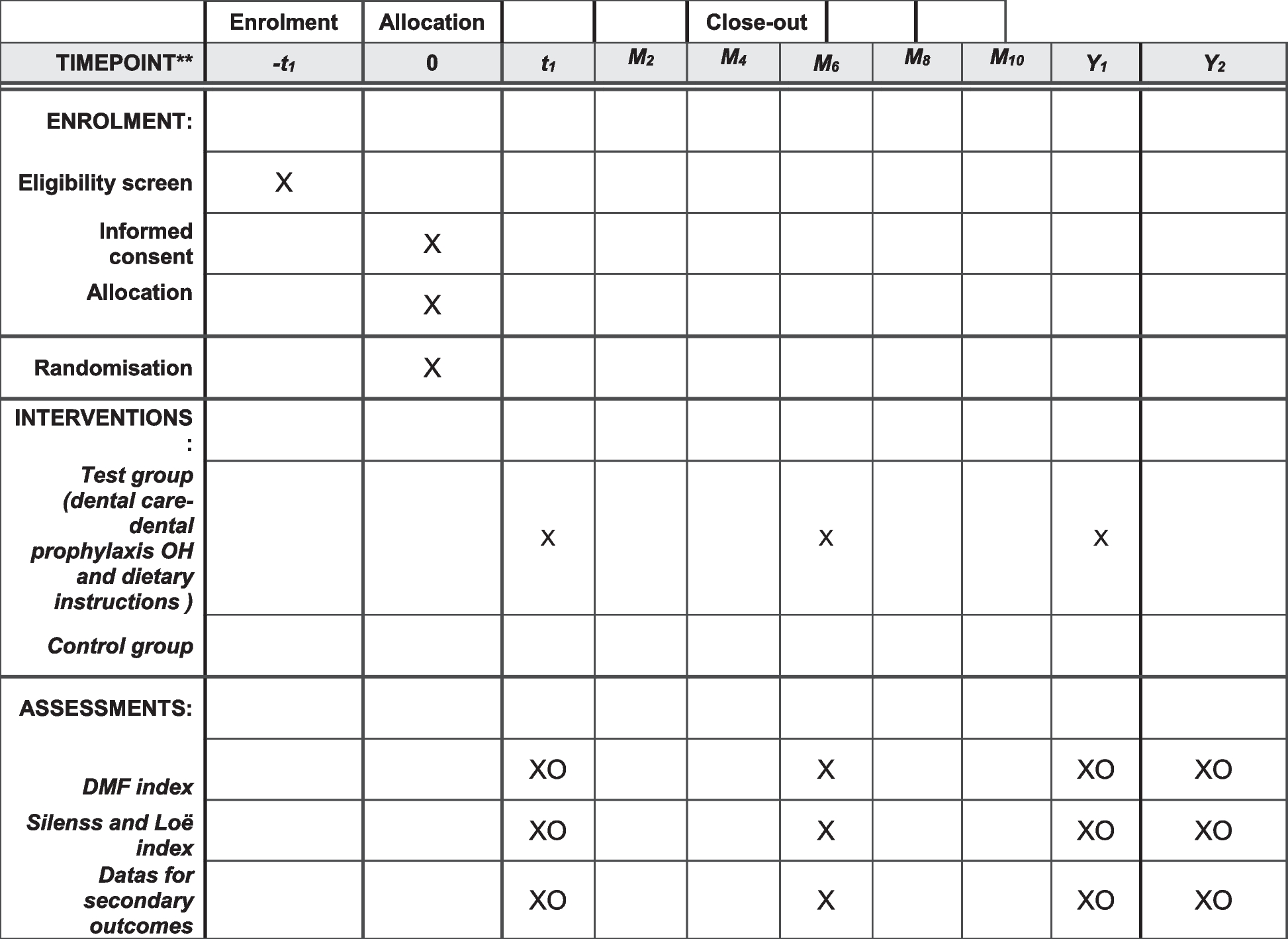
The prevalence of post-bariatric surgery depression is high reaching up to 64.9% [31], which may reduce their adherence to the trial. Moreover, a retrospective chart review including data from 1020 consecutive bariatric surgery candidates indicated a rate of previous suicide attempts of 11.2% [32]. We focus on education and helping patients become their own best advocates. On the other hand, to foster the study and increase the interest of participants, we will recruit three patients to voluntarily join our data collection in the 30-day follow-up by phone. This approach may be a viable tool for improving the compliance of other patients since they are all the participants in this trial. As a result, we will thank these three patients in private. The complete time schedule for enrolment, intervention and assessment is shown in Fig. 2.
Fig. 2
Schedule of enrolment, interventions, and assessments. POD, postoperative day; LUS, lung ultrasound; RMs, recruitment manoeuvres; SpO2, peripheral oxygen saturation, FiO2, fraction of inspired oxygen; ICU, intensive care UNIT
Data monitoringParticipant’s data will be collected through the CRF. The protected folder will be backed up once a month. Informed consent and trial end dates will be recorded. All changes made to the raw data and all steps taken in the analysis will be recorded in the CRF and IBM SPSS. A data monitoring committee is not considered as this is a low-risk intervention.
留言 (0)