
記住我






A 55-year-old white female presented as a referral for pain, visual decline, diffuse intraocular inflammation and a newly identified lesion of the right ciliary body. She reported one month of new floaters in the right eye and increased light sensitivity. The patient’s past medical history was significant for cutaneous melanoma diagnosed in 2018 with more recent testing demonstrating metastatic involvement of the post-auricular skin, lung, and brain. The patient had undergone three cycles of external beam radiation to the brain and one round of combination nivolumab and ipilimumab shortly prior to presentation.
On the initial exam, the patient’s visual acuity was measured to be 20/200 in the right eye and 20/20 in the left eye. Both pupils were equally reactive without an afferent pupillary defect. Intraocular pressure was measured to be 28 mmHg in the right eye and 18 mmHg in the left eye. Slit lamp examination of the right eye demonstrated an inferior pseudo-hypopyon with 1–2 + cell and flare. Pigmented cells covered the iris surface and seeded the angle for 360 degrees on gonioscopy. Posterior synechiae were present. A minimally pigmented ciliochoroidal mass was visible nasally with overlying sentinel vessels. Pigmented vitreous cells were present on posterior examination. The retina was otherwise normal (Fig. 1). Examination of the left eye was unremarkable. B-scan ultrasound of the right eye showed a homogeneous ciliochoroidal mass measuring 8.2 mm x 13.7 mm x 12.5 mm (Fig. 2).
Fig. 1
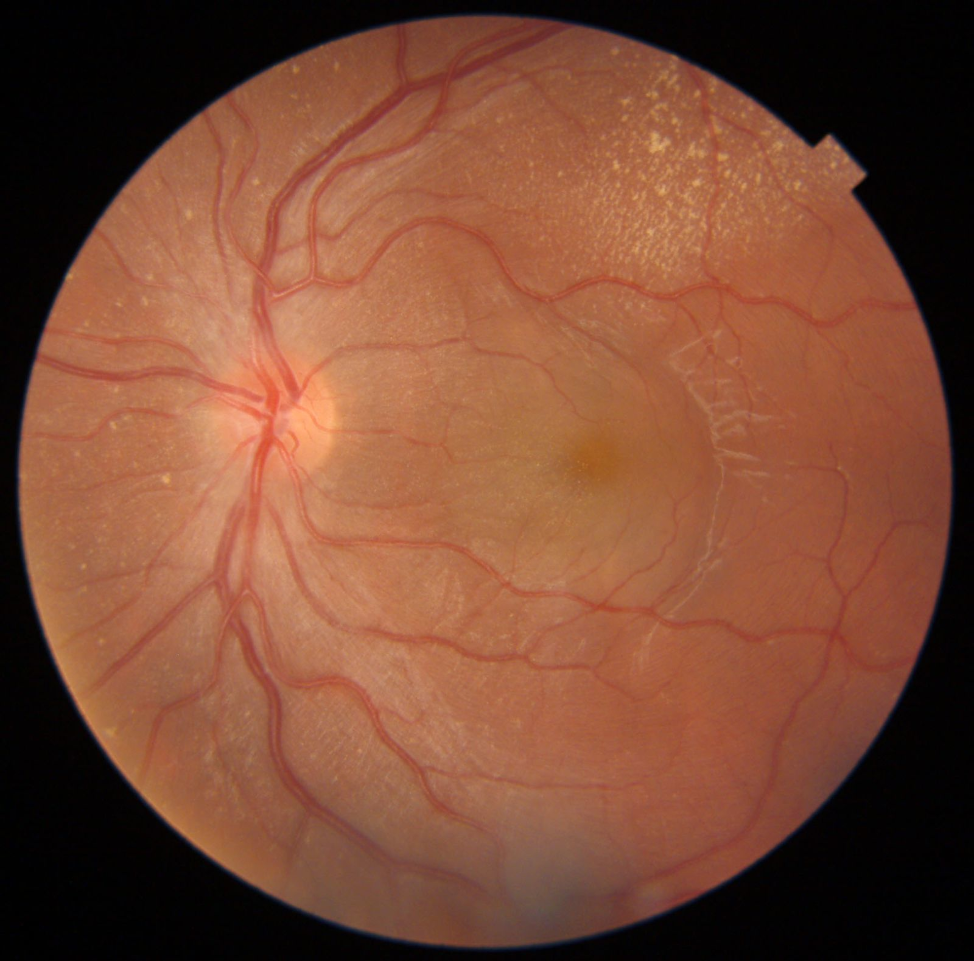
A Slit lamp photograph of the right eye. Note a nasal amelanotic mass originating from the ciliary body with overlying sentinel vessels visible in the retrolental anterior vitreous with pseudo-hypopyon in the anterior chamber. B Fundus photography shows a mildly pigmented ciliary body with vitreous cell. The optic nerve and macula appear normal
Fig. 2
B-scan ultrasound of the right eye on initial presentation. Note a peripheral homogeneous choroidal mass measuring 8.2 mm x 13.7 mm x 12.5 mm
Our exam findings and the patient’s medical history of primary cutaneous melanoma led to concerns of intraocular metastasis. Given the size of the tumor and extent of anterior chamber and angle seeding, the patient chose to enucleate the right eye. In pre-operative holding one week later and two weeks after her first infusion of nivolumab and ipilimumab (1 mg/kg and 3 mg/kg, respectively), the tumor was noted to have regressed markedly, the anterior chamber seeding had cleared, and vitreous cell diminished. The surgery was subsequently deferred. Follow up in the clinic demonstrated tumor measurements of 1.8 mm x 9.7 mm x 8.0 mm on B-scan ultrasound (Fig. 3). The patient’s vision in the right eye had improved to 20/60 and intraocular pressure was 13 mmHg. On slit lamp exam, the pseudo-hypopyon had dissipated and the ciliochoroidal mass had regressed and was no longer visible (Fig. 4). The patient remained on systemic therapy with standard dosing of 1 mg/kg nivolumab and 3 mg/kg ipilimumab. Her subsequent follow up exam demonstrated complete regression of the ciliochoroidal mass (Fig. 5). One year later, her visual acuity remained 20/60 limited by posterior lens capsule changes and dilated exam demonstrated a grossly normal retina. She is currently without evidence of disease.
Fig. 3
B-scan ultrasound of the right eye on follow up exam. Note a reduction in mass now measuring 1.8 mm x9.7 mm x 8.0 mm
Fig. 4
Slit lamp photograph of the right eye on follow up exam. Note regression of the ciliary body mass with resolution of the pseudo-hypopyon
Fig. 5
B-scan ultrasound of the right eye after treatment with ipilimumab and nivolumab. Note a complete regression of the ciliary body mass
Discussion and conclusionsThe differential for a new intraocular mass includes primary tumors of the eye or metastatic disease with secondary intraocular involvement. Differentiating between the two can be challenging and requires a complete review of medical history, a thorough examination of the eye, and additional testing including but not limited to ocular ultrasound, fundus autofluorescence, and fluorescein angiography [3]. In adults, metastatic disease represents the most common intraocular lesion [3]. Breast (40–53%) and lung (20–29%) are the most common sources of metastatic intraocular disease [3]. The choroid presents the most common site of metastatic spread (40–46%), largely due to the high vascularity and associated blood supply [1, 3, 4]. The less commonly involved iris and ciliary body are affected in approximately 9% and 2% of cases respectively [3]. One case series identified ciliary body involvement in two out of 14 cases compared to 11 out of 14 cases with choroidal involvement [4]. On presentation, initial symptoms of metastatic disease may include decreased vision, eye pain, photopsia, floaters, diplopia, and other visual change depending on site of involvement [1, 3].
Cutaneous melanoma is an increasingly common skin cancer and the leading cause of death from cutaneous malignancy [1]. It has a predilection to spread hematogenously to the lungs, liver, skin, and brain [1, 5]. Cutaneous melanoma represents a rare source of intraocular metastatic disease with studies suggesting it comprises less than 5% of ocular metastasis [1, 5]. Long term survival in metastatic cutaneous melanoma remains poor, with the reported 5-year survival rate approximately 22% [1, 5]. When it does involve the eye, diagnosis can be challenging if primary disease has not been identified and findings can mirror that of primary uveal melanoma [5]. In these cases, genetic testing can assist in differentiating the two pathologies [5]. We deferred genetic test in our patient as she had a known history of metastatic cutaneous melanoma.
Our patient presented with a known history of cutaneous melanoma diagnosed 5 years prior to presentation of ocular metastatic disease. This interval is consistent with literature identifying that 72% of patients who developed ocular metastasis did so within 5 years of diagnosis of primary cutaneous disease [1]. Prior to presentation, she had received one cycle of combination immunotherapy with nivolumab and ipilimumab. Examination of the patient’s right eye demonstrated a large, mildly pigmented ciliochoroidal mass with direct invasion and seeding of the angle along with prominent anterior and posterior segment inflammation. B-Scan ultrasound showed a solid homogeneous ciliary body/ choroidal mass associated with vitreous debris. These findings could be interpreted as primary uveal melanoma; however, the associated clinical findings of anterior chamber and vitreous seeding favored a metastatic cutaneous melanoma in keeping with our patient’s medical history. Surgical treatment with enucleation of the right eye was elected given the extent of disease; however, on the day of surgery her tumor was noted to have regressed significantly, and surgery was deferred. Subsequent follow up examinations documented complete regression of the ciliochoroidal tumor following treatment with combination of nivolumab and ipilimumab.
Ipilimumab and nivolumab represent fully humanized monoclonal antibodies targeting inhibitory checkpoints of T-cell activation and have been approved by the US Food and Drug Administration for a variety of tumors including metastatic melanoma [2]. Ipilimumab targets cytotoxic T lymphocyte antigen-4 (CTLA-4) expressed on T-cells. CTLA-4 interacts with B7 to inhibit T-cell activation and proliferation; by inhibiting this process, ipilimumab activates T-cells with subsequent targeting of tumor cells [2]. Similarly, nivolumab targets programmed cell death protein 1 (PD-1) to prevent inhibition of T-cell proliferation, differentiation, and cytokine secretion [2]. Use of ipilimumab and nivolumab combination therapy has demonstrated improved median progression-free survival relative to either treatment independently in metastatic melanoma [2, 6]. The 3-year survival rate has improved to 58.3% with this regimen [7].
Recent reports have documented patients with cutaneous metastatic melanoma and good systemic response following immunotherapy who subsequently develop intraocular metastatic disease, suggesting ocular immune privilege may limit utility in the treatment of ocular metastasis with dual checkpoint inhibitors [7, 8]. However, a 2019 case report by Fernandez-Diaz, et al., documented a patient with metastatic cutaneous melanoma with vitreous involvement treated with combination nivolumab and ipilimumab with complete response at the ocular level [9]. A subsequent case series by Francis, et al., documents 14 eyes in 11 patients with cutaneous melanoma metastatic to the vitreous, of which ten patients received checkpoint inhibitor therapy; three of the 14 eyes had improved visual acuity following treatment [10].
Our case supports the evidence reported by Fernandez-Diaz, et al., by demonstrating complete regression of intraocular metastatic disease of cutaneous melanoma with combination ipilimumab and nivolumab. In contrast to their case, we present a larger and more aggressive intraocular lesion with ciliochoroidal involvement, direct invasion of the angle, and seeding of the anterior chamber and vitreous cavity. Additionally, our case demonstrated complete regression following dual checkpoint inhibitor therapy and did not require additional vitrectomy to improve vision.
In conclusion, management of metastatic cutaneous melanoma patients can be complex and often requires a multidisciplinary approach. Combination therapy with ipilimumab and nivolumab immunotherapy has been shown to be effective in the treatment of aggressive intraocular metastatic cutaneous melanoma.
留言 (0)