Coats’ disease is an idiopathic retinal vasculopathy that is non-hereditary in its nature. It is characterized by telangiectasia and aneurysm of retinal vessels, intraretinal and subretinal exudation, and exudative retinal detachment [1,2,3]. Coats disease is more common in Caucasian [7]. However, there are few studies of Coats’ disease based mainly in Asian populations. One of those studies was done on Korean patients, 45% of those having childhood-onset disease, mean age at presentation was 8.6 years (range 0.2–17.8) and 55% of those having adult-onset disease, mean age at presentation was 39.8 years (range 18.3–69.0) [8].
Coats’ disease commonly presents unilaterally with strong male predominance [5]. Herein, we present a case of a 20-year-old female, which is unusual because male predominance is a regular feature of the disease in the literature [5, 9,10,11]. However, a recent extensive study of 351 eyes of 351 instances of Coats’ disease from a single hospital revealed that 56 cases (16%) were female [7]. Therefore, despite the fact that it is uncommon to identify coats’ disease in females, it still can be detected.
Our patient presented with a gradual, painless decrease in her left-eye vision. The IOP was normal. The slit lamp examination was also normal, with no evidence of any rubeosis. In the literature, decreased vision is the most common complaint [12, 13]. Unusual symptoms such as discomfort, vitreous hemorrhage, anterior segment abnormalities, and elevated IOP can also present [13]. However, in adults-onset coats’ disease, a subset of patients remain asymptomatic for an extended period of time and are diagnosed on routine fundus examinations [2, 4].
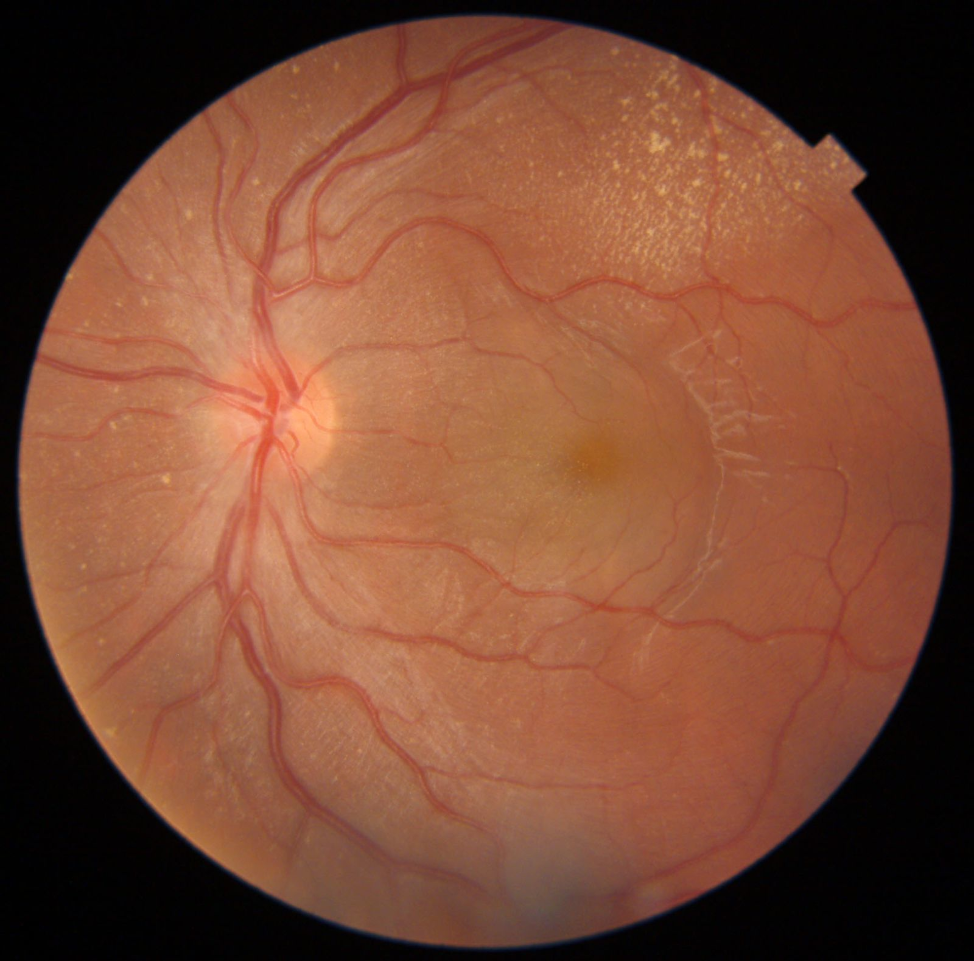
Indirect ophthalmoscopy fundus examination is the gold standard for diagnosing Coats’ disease [5]. Every case reveals retinal telangiectasia, which typically has a fusiform shape. The most frequently affected quadrants are the inferior and temporal ones [5, 14]. Nearly all cases have intraretinal exudation, which can be widespread and extend far from the telangiectasia [5]. Additionally, the density of macular exudate serves as a significant indicator of visual prognosis besides poor vision at presentation, even with appropriate treatment [1, 7]. In our case, the patient had inferotemporal telangiectasia that is sausage-like in shape with large aneurysms, extensive exudate in all 12 clock hours involving macula, extensive macular edema, and exudation, which align with the typical presentation with poor prognostic factors. However, the patient’s results after the treatment were good, and the patient’s vision improved.
Shields classified Coats disease into five stages: stage 1, which only shows retinal telangiectasia; stage 2, which shows both telangiectasia and exudates; stage 3, which shows the development of exudative retinal detachment; stage 4, which shows total retinal detachment and glaucoma; and stage 5, where the disease has progressed to the end stage and is occasionally accompanied by phthisis bulbi [1, 7]. We classified our patient as stage 3 due to the observation of retinal detachment. However, this is not concordant with the previous studies that report that nonjuvenile cases of Coats’ disease are usually diagnosed at stage 2 [7].
The treatment modality for coats’ disease depends mainly on the severity of the disease, and it always aims to preserve vision and ocular anatomy [1, 6]. Cryotherapy, laser photocoagulation, scleral buckling, external subretinal fluid drainage, and pars plana vitrectomy (PPV) are among the treatment options. We have also utilized adjunctive intravitreal injections of corticosteroids and anti-VEGF in patients with subretinal exudates and macular edema. Ocular VEGF levels have been shown to be elevated in patients with Coats’ disease. This finding has prompted the use of anti-VEGF therapy as both primary and adjuvant treatment [7, 15]. Laser photocoagulation and cryotherapy are the first-line treatments for Coats’ disease, particularly for stage 1. However, stages 2 to 3 A do not respond well to these treatments when used independently because retinal exudative changes and serous retinal detachment obstruct the effectiveness of laser therapy. To drain subretinal fluid before photocoagulation, surgical intervention might be necessary, or alternatively, anti-VEGF injections as adjuvant therapy might prove effective [16].
Our patient had extensive retinal exudation with massive subfoveal fluid and exudate, so the decision was made to initiate treatment with intravitreal Aflibercept injections. A reduction in subretinal fluid, a decrease in the size of telangiectatic vessels, improved retinal detachment, and improved visual acuity were observed. Kang et al. [8] reported that the use of more frequent anti-VEGF injections during the initial treatment period was associated with an improvement in final visual acuity by approximately 9.4 letters.
While multiple recent reports have demonstrated resolution of severe retinal detachments following anti-VEGF therapy [17], a study by Ramasubramanian et al. [18] cautioned against the use of anti-VEGF agents due to the development of vitreoretinal fibrosis and tractional detachments in eight pediatric patients. Another study by Daruich et al. [19] showed that 40.6% of 69 patients exhibited findings associated with extramacular fibrosis, which were not linked to cryotherapy, laser therapy, or anti-VEGF treatment.
Recurrences can also occur several years later, characterized by the return of exudates after the disease appears to have successfully remitted. A side consequence of Coats disease could be cataract development [20]. Therefore, even once the disease has stabilized, we advise close patient monitoring due to potential consequences and recurrences. Patients typically schedule lifetime follow-up appointments, ideally once every six months [21].






留言 (0)