Currently, the ICL is the most commonly used PIOL; however, there are visual quality problems owing to its central hole design and limited range of correction. Most previous studies on PRLs have demonstrated their short- and long-term effectiveness and predictability. Their suspension design avoids contact between the PRL and the anterior surface of the lens, thereby reducing the risk of cataracts and ensuring IOP stabilization. However, current PRLs still have many complications that require further improvement. In this study, a self-controlled experiment in rabbit eyes with PRL-S5 and conventional PC-PRLs was performed to observe in vivo safety 1 year postoperatively.
Secondary cataract is a common complication of posterior chamber IOLs that occurs mainly from inflammation resulting from contact between the PRL and its lens, leading to lens epithelial cell (LEC) metaplasia and migration. Another reason is metabolic damage from changes in aqueous humor dynamics. The PRL suspension design avoids the need for continuous contact between the pIOL and any specific area on the anterior surface of the lens. Therefore, the incidence of cataracts was lower than that of other posterior chamber types of IOLs [14]. The results of a meta-analysis showed that the incidence of postoperative cataracts in Chiron-Adatomed PIOL, ICL, and PRL was 25.66%, 8.48%, and 3.59%, respectively. Seven eyes in the PRL group had cataracts, of which six developed cataracts as a result of intraoperative trauma and the other eye developed cataracts 24 months postoperatively [16].
In our study, mild anterior subcapsular opacification of the crystalline lens appeared in the PC-PRL, beginning in the third postoperative month (12 weeks) and progressing gradually thereafter. PRL S5 developed opacification later and progressed slower than PC-PRL; however, there was no significant difference between the two in terms of the microscopic manifestations of histology at 1 year. Six weeks postoperatively in the rabbit eye is equivalent to 2 years postoperatively in the human eye. The overall observation time in our study amounted to 1 year, approximately 52 weeks, which is equivalent to 10 years for the human eye [17]. According to the morphological classification of cataracts, punctate ASC, which is usually non-progressive, may be associated with surgical trauma. Diffuse, annular, and centrally dense ASC, in contrast, progresses slowly and may be related to the impaired metabolism of the lens epithelium and mechanical damage caused by a vault that is too low [9]. The fact that the ASC in the present study occurred in the long-term period after surgery (12 weeks) and that both groups had a gradual progression with predominantly annular and diffuse shapes, suggests that the chordal design improved the flow of atrial fluid to a certain degree and maintained the metabolism of the crystalline lens over a longer period. However, an inflammatory response may still occur in contact with crystalline lens, ultimately leading to cataract development.
IOP is an important safety indicator. In our study, IOP was regularly measured in each group, and the results indicated that IOP in both groups stabilized within the normal range in rabbit eyes after 1 week. The IOP in anesthetized rabbits is 16 ± 2.1 mmHg (8.4–23.3) [18]. The increase in IOP after PRL surgery was associated with common postoperative events such as viscoelastic retention or reactions to steroid medications. In a previously published short-term PRL experiment, IOP returned to normal on the third day post-surgery but increased again on the 10th and 15th days post-surgery. However, in the short-term postoperative period, there was no significant difference in IOP among the different PRL designs [19]. The increase in IOP observed in that study may have resulted from reactions to steroids. In our study, steroids were used for three weeks post-surgery, and all rabbit eyes showed an IOP increase only on the day of surgery owing to viscoelastic retention. The IOP remained stable at 1 week, 3 months, 6 months, and 1 year post-surgery. This indicates that the sinusoidal drainage groove design of the new-generation PRL maintained a stable IOP without the need for iridotomy, resulting in a low risk of postoperative glaucoma and long-term safety.
The relationship between IOP and postoperative refraction was another worth noting point, which was mentioned by previous studies. The predicted refractive difference per 10 mm Hg IOP decrease was + 0.15 to 0.50 Diopter [20, 21]. Therefore, the potential risk of postoperative hyperopic shift should be taken into account when performing biometric measurements for IOL power calculation in patients with abnormally elevated IOP. Since this study was an animal study, the lens power calculation was not considered. Over the years, numerous IOL power calculation formulas have been developed to achieve the most accurate postoperative refractive outcomes [22]. PRL was a posterior chamber phakic intraocular lens. The Van Der Heijdei and Holladay formula has historically been used to calculate phakic lens power [23, 24]. Nowadays, artificial intelligence intraocular power calculation formular has been explored [25]. The PRL lens power calculation will be explored in the future research.
In this study, one rabbit eye experienced PRL dislocation in the anterior chamber, likely resulting from suboptimal placement during surgery. Previous studies reported an in-situ rate of 16.7% for small-sized PC-PRL (12.3 mm in diameter) and 100% for large-sized PC-PRL (13.3 mm in diameter). The in-situ rate for PRL S5 (13.3 mm in diameter) was 87.5%, with one case of dislocation on the 10th day post-surgery; however, the authors were unclear about the cause of this dislocation [14]. It is important to note that the rabbit eyes used in this study were not a high-myopia model, and the condition of the zonules was not reported. In addition, the OCT used in this study did not reveal the zonules. The contact between the PRL haptics and zonules may weaken zonular tension. The significant increase in tension on zonular fibers owing to axial elongation makes these fibers particularly fragile in patients with high myopia [12]. This can lead to zonular rupture and spontaneous dislocation of the PRL into the vitreous cavity [13, 26]. Therefore, further studies are required to enhance the implantation stability of PRL S5. Moreover, studies on optical quality and visual performance should be conducted to determine the long-term safety and effectiveness of this intraocular lens implant.
In our study, one eye exhibited corneal edema 1 week postoperatively, which may have resulted from intraoperative damage to the corneal endothelium, leading to endothelial decompensation. A transient episodes of elevated IOP often occur immediately after surgery due to residual viscoelastic materials. However, as the inflammatory response diminished, the IOP normalized, and no subsequent elevation in IOP was observed during follow-up. Additionally, one eye developed scleral staphyloma 3 months postoperatively, although the precise etiology remains uncertain. Both rabbit eyes experienced severe ASC, yet no increase in IOP was detected during the follow-up period.
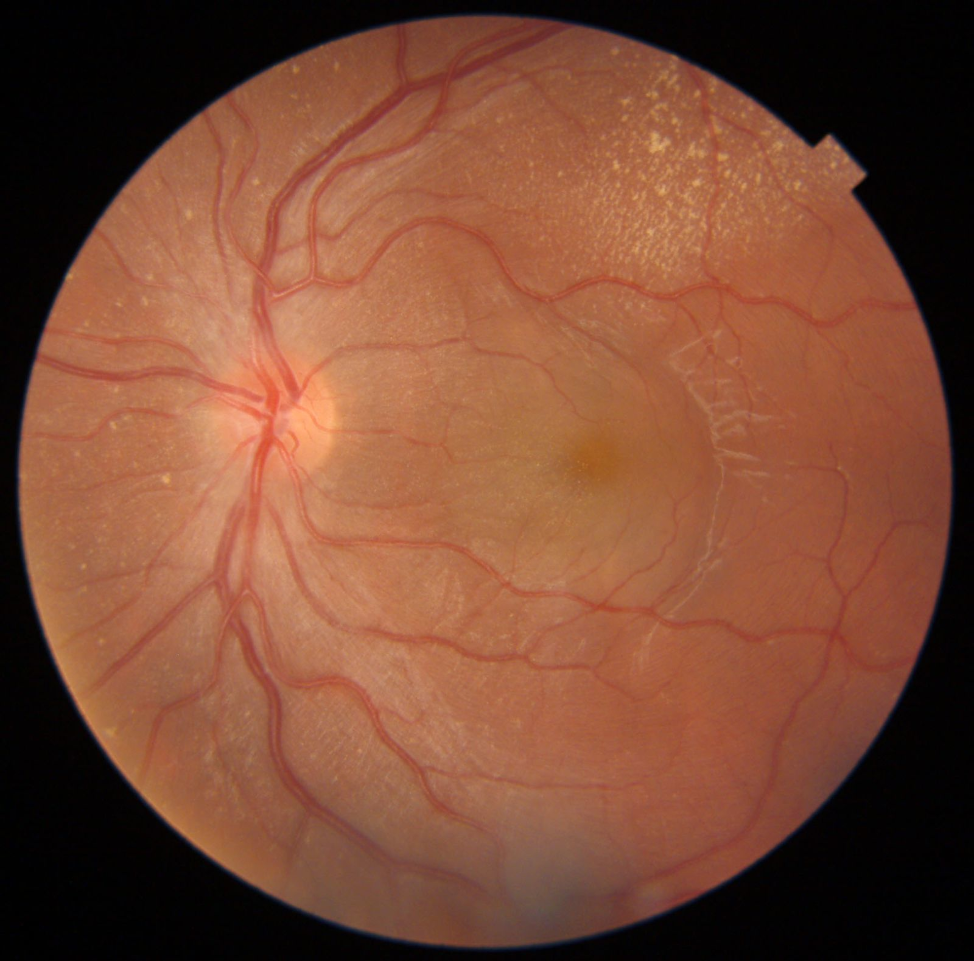
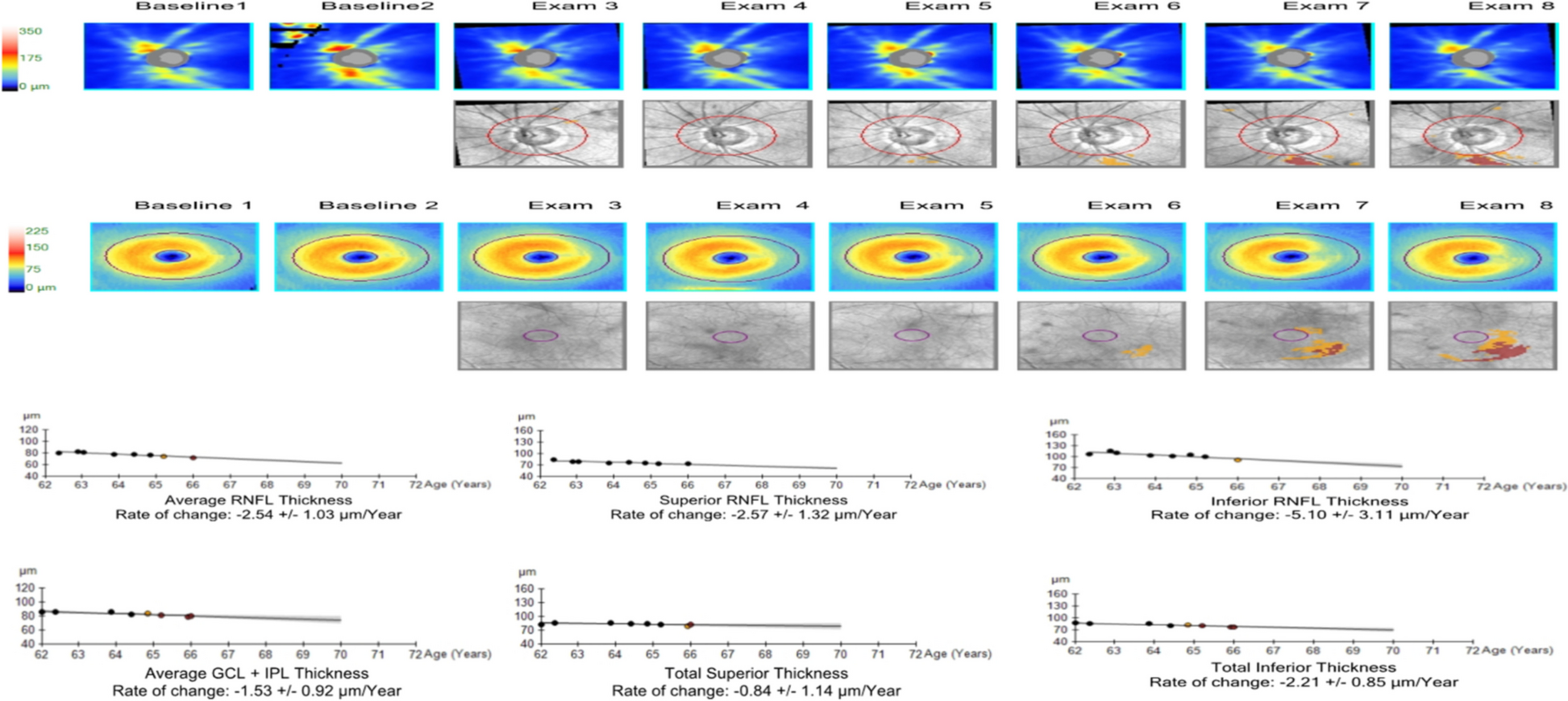
Our study has several limitations. First, the sample size was relatively small, consisting of only four rabbits. The difference of opacification area between two groups of PRL was not significantly. conclusions need to be justified by larger sample sizes in the future. Second, no blank control group was included. However, the primary objective was to assess the safety of the novel PRL design, and the material of the PRL had already been validated, making a comparison with non-implanted rabbits unnecessary. Third, we did not report on the long-term impact of the PRL on corneal endothelial cell density (ECD). The ECD is a regular postoperative follow-up examination performed in clinical practice. The PRL is a posterior chamber PIOL that effectively avoids contact with corneal endothelial cells, and previous clinical applications have demonstrated its minimal effect on the corneal endothelium. The measurement of ECD in the rabbit eye was difficult; thus, it was replaced with a slit-lamp examination of the cornea. A detailed assessment of the endothelial cell status and provide a more comprehensive evaluation of the long-term effects on the cornea. Additionally, the rabbit eye model does differ from humans, which may restrict the application on human eyes. Rabbit corneal endothelial cells can regenerate, unlike those in humans [27]. Considering that the rabbit eye is closer in size to the human eye and is easier to perform ophthalmic surgical operations and observation, we used a rabbit eye model. We are willing to further observe the effect of PRL on corneal endothelial cells in future studieAs. Finally, previous studies have documented other potential complications associated with PRL, including secondary uveitis, retinal detachment [28], and choroidal neovascularization [29]. While IOP was stable postoperatively, this does not fully rule out the risk of glaucoma. Structural changes or damage to the optic nerve could still occur without elevated IOP, The retina and vitreous were not observed in our study. In future study, we will assess the optic nerve fiber to better evaluate the potential risk of glaucoma, and evaluate the retinal and uveal safety profile PRL thoroughly.






留言 (0)