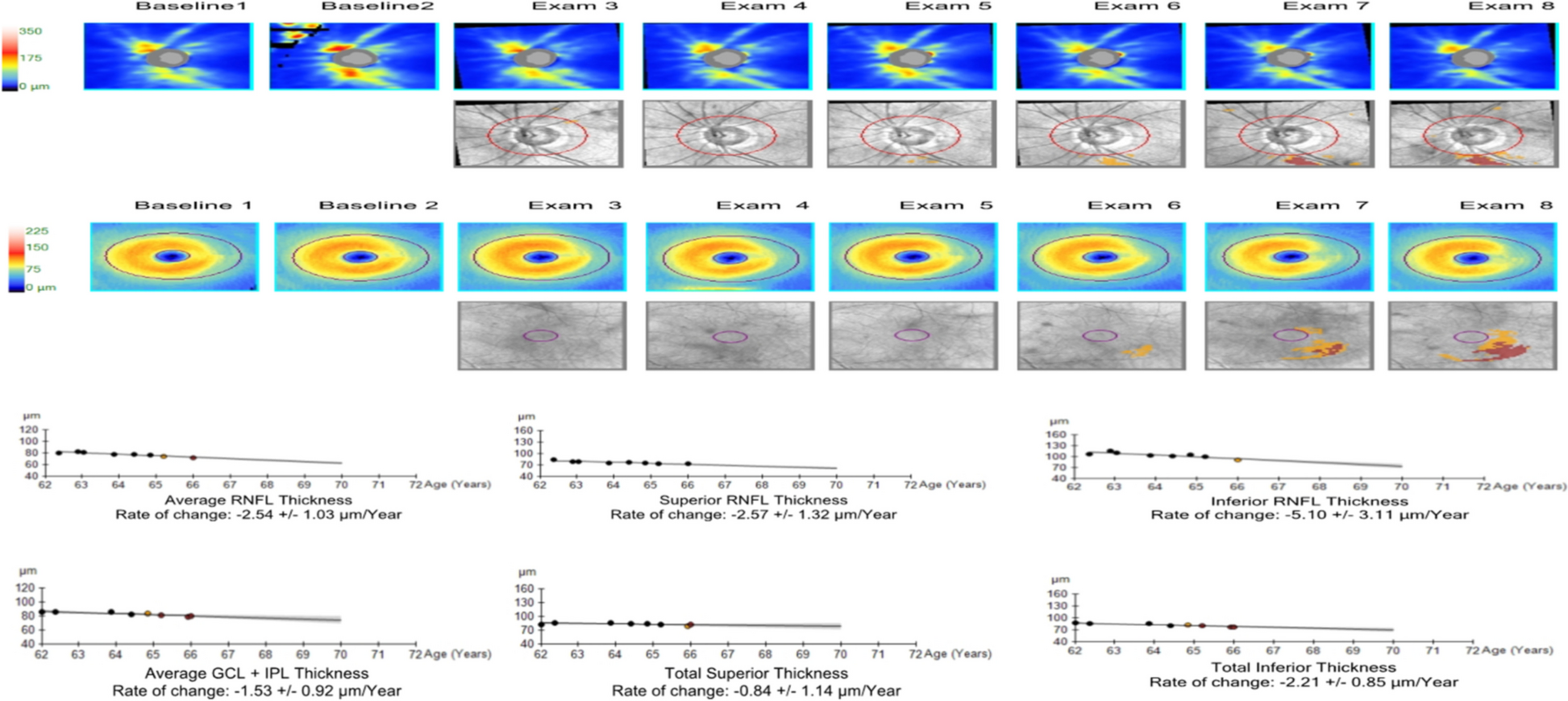
In this study, we utilized the Graduated Progression Analysis software of Cirrus HD-OCT to compare the thinning rates of GCIPL and RNFL among normal, POAG, and pseudo-exfoliation glaucoma (PXG) eyes. Our findings indicate that average RNFL and GCIPL thinning rates in PXG patients were faster than those seen in POAG patients and the control group. Moreover, both RNFL and GCIPL thinning rates in POAG patients were significantly higher compared to the control group. Interestingly, GCIPL and RNFL thinning rates were found to be positively correlated in PXG patients. However, within both types of glaucoma, there was no significant difference in the GCIPL and RNFL thinning rates between mild and moderate-severe groups.
Evaluating structural optic nerve and ganglion cell layer damage is vastly important in diagnosing and monitoring patients with glaucoma. With new OCT technologies, automated quantitative and reproducible measurements of the optic nerve head, RNFL, and GCIPL have become feasible. Disease progression detection is also key in the follow-up and treatment of glaucoma and can be detected using software incorporated into new OCT devices. Several studies have examined the thinning rates of RNFL, macular thickness, and macular volume changes for glaucoma progression detection using various OCT devices [15,16,17]. Additionally, the rate of thinning of inner retinal structures in glaucoma patients has been assessed using OCT device software, highlighting that ganglion cell destruction plays a crucial role in glaucoma pathogenesis [14, 18,19,20,21,22]. Numerous studies have evaluated GCIPL and RNFL thinning rates in both the general population and glaucoma patients. Belghith et al. reported a GCIPL thinning of −0.11 µm/year for healthy individuals and −0.18 µm/year for POAG patients using Spectralis OCT [18]. Recently, Hammel et al. and Lee et al. respectively reported GCIPL thinning of −0.14 µm/year and −0.31 µm/year, and RNFL thinning of −0.48 µm/year and −0.60 µm/year in healthy eyes using Cirrus HD-OCT. They also documented rates of −0.57 µm/year and −0.49 µm/year GCIPL thinning, and −0.98 µm/year and −0.90 µm/year RNFL thinning in POAG eyes [14, 20]. In our study, we observed −0.23 µm/year GCIPL thinning in normal eyes, −0.64 µm/year in POAG eyes, and −1.06 µm/year in PXG eyes using Cirrus OCT software. Also, we noted −0.33 µm/year RNFL thinning in normal eyes, −0.86 µm/year in POAG patients, and −1.33 µm/year in PXG patients. Lee et al. reported −1.46 µm/year GCIPL thinning and −1.31 µm/year RNFL thinning in PXG patients [14].
Some differences distinguish our study from past research. The disparity in results between our study and others could be attributable to the ethnic diversity, average age, and the variety of OCT devices’ segmentation algorithms. The subjects of our study were of the same race, and there was no statistically significant divergence in demographic characteristics among the groups. In the research by Hammel et al., the majority of the participants were of European and African descent, whereas in the study by Lee et al., the subjects were East Asian (Korean); our subjects, however, were Caucasian (Turkish). The differing outcomes may stem from variations in axial lengths and the prevalence of myopia among East Asians. An elongated globe in myopia-afflicted eyes, which results in a larger retinal surface area and a thinner GCIPL, has been documented [23].
The prognosis of glaucoma is generally poorer in patients with pseudo-exfoliation glaucoma (PXG) due to an unfavourable response to medical therapy [11, 24]. However, there was no significant difference in the IOP among the control group, POAG patients, and PXG patients at the time of enrollment in the study (p = 0.836). Despite this, the most rapid progression was observed in PXG patients. These findings suggest that non-IOP-related factors, such as vascular alterations, neurodegenerative conditions, or anatomical variances – which can be observed in PXG patients – could contribute to glaucoma progression [25,26,27]. Consequently, eyes with PXG should be treated more aggressively than those with POAG. Moreover, even though IOP was well-managed in POAG patients, it displayed a quicker progression compared to the control group.
We hypothesize that the non-IOP-related factors mentioned above for PXG patients may also be effective in POAG patients, thus necessitating close monitoring.
We performed a sub-analysis, dividing POAG and PXG eyes into two subgroups based on the degree of VF involvement (MD > −6.00 for mild vs. MD < −6.00 for moderate-severe) and then investigated the impact of glaucoma severity on RNFL and GCIPL thinning rates. Nguyen et al. likewise studied the influence of the glaucoma stage on its progression. However, their study differed from ours as their glaucoma patients had various types of the condition. These patients were classified into three groups: mild, moderate, and severe stages. They discovered that the average, superior, and inferior RNFL and GCIPL thinning rates were consistent across the glaucoma stages [28].
Shin et al. divided POAG patients into two groups – mild and moderate to advanced – based on their MD values in their study. They found no significant difference in the GCIPL thinning rate between the groups in the GPA program. However, the RNFL thinning rate was significantly less in patients with moderate to advanced glaucoma. The researchers attributed this to the floor effect, which they believed prevented further RNFL thinning. They also proposed that RNFL measurements may not be useful for monitoring glaucoma progression in advanced patients [29]. In contrast, we found no significant difference in GCIPL or RNFL thinning rates between mild and moderate-severe groups in both POAG and PXG. We suspect that this discrepancy may be due to the higher baseline RNFL and GCIPL thicknesses in our study.
Because the pathophysiology of glaucoma is not fully understood, determining whether the loss of macular ganglion cells and axons occurs simultaneously, or if one precedes the other, is challenging. It is feasible that, in glaucoma patients, the thinning of peripapillary RNFL and macular GCIPL occurs at different stages during the disease’s progression [20]. In this study, we found no correlation between GCIPL and RNFL thinning rates in the control group. However, in POAG patients, we observed a correlation between average GCIPL thinning rates and average RNFL thinning rates, as well as between superior GCIPL thinning rates and both superior and inferior RNFL thinning rates. Interestingly, we discovered that GCIPL and RNFL thinning rates were correlated in all quadrants in PEXG patients. This implies that macular ganglion cell loss was correlated with the loss of their axons as the rate of glaucomatous damage increased. Therefore, we propose that earlier surgical treatment should be considered in patients with this correlation.
Our study has certain limitations. Firstly, we were unable to assess glaucoma progression on OCT in conjunction with progression on VF testing due to the need to replace the standard automatic perimetry device during follow-up. Secondly, we did not evaluate the natural course of untreated glaucoma as we excluded patients who had undergone follow-up glaucoma surgery, focusing solely on those receiving anti-glaucoma treatment. Notably, measurements of glaucoma patients were conducted while patients were using various topical anti-glaucoma drugs for different durations. The influence of these medications on ganglion cells remains undetermined. Lastly, as our study is retrospective and of a restricted Caucasian population, our findings may not be universally applicable. Further studies involving larger groups will be needed to enhance our understanding of the disease course in various types of glaucoma.






留言 (0)