
記住我


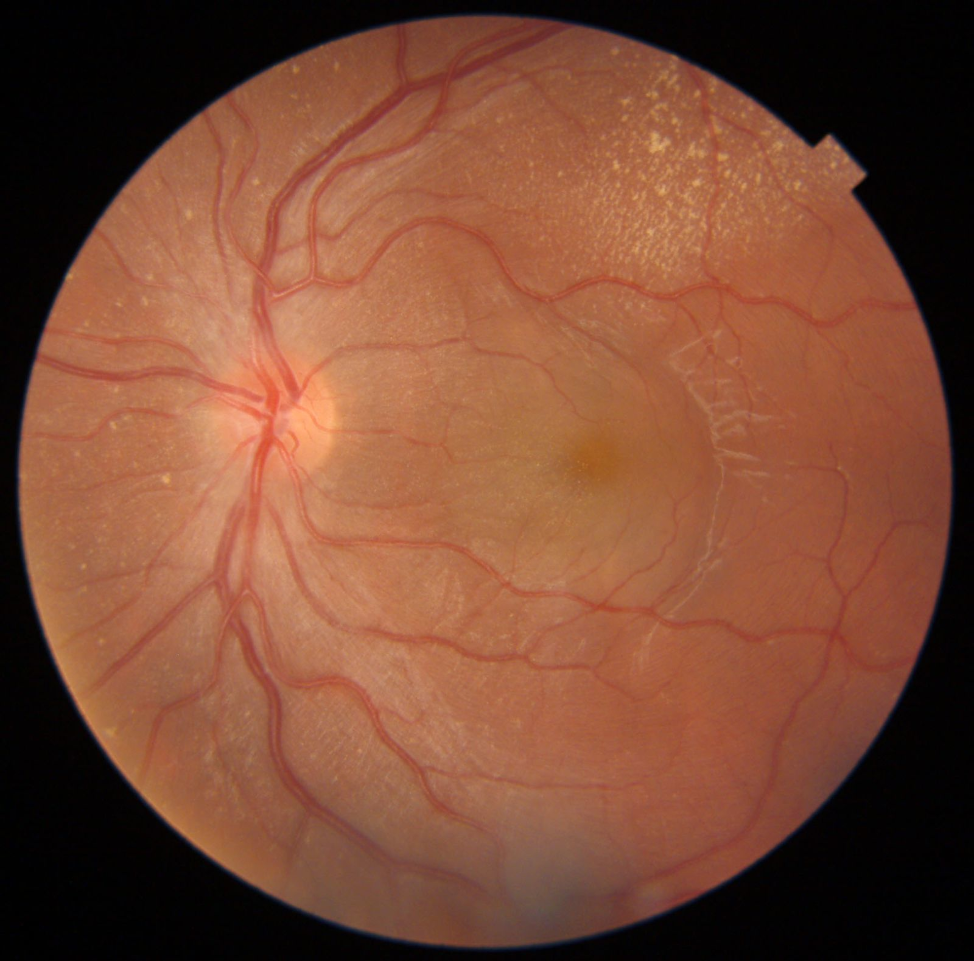



A 43-year-old healthy male with no prior history of systemic diseases, including hypertension or diabetes mellitus, presented at the retina clinic with a sudden onset of decreased vision in his left eye, noted since the previous evening. Visual acuity was measured at 6/6 in the right eye and 6/120 in the left eye. Anterior segment examination and intraocular pressure were normal in both eyes. A dilated fundus examination of the right eye revealed no significant abnormalities; however, the left eye exhibited a well-defined, boat-shaped premacular hemorrhage with a fluid level, characteristic of a subhyaloid hemorrhage. Upon careful inspection, a ‘double ring sign’ was identified, indicating sub-ILM involvement. Additionally, a clump of deep red, coagulated blood was positioned anterior to the fovea, and there were scattered deep blot retinal hemorrhages of varying sizes throughout the fundus (Fig. 1a).
Fig. 1
Colour fundus photograph and optical coherence tomography scan of the premacular hemorrhage: a, b: The left eye revealed a well-defined pre-macular hemorrhage with a fluid level and presence of a ‘double ring sign’ (red arrow indicates the subhyaloid space and blue arrow indicates the sub-internal limiting membrane [ILM] space). Inside the hemorrhage cavity, a clump of deep red, coagulated blood (orange arrow) was found in front of the fovea. Scattered deep blot retinal hemorrhages (yellow arrows) of various sizes were found throughout the fundus. Optical coherence tomography confirmed the hemorrhage as a sub-ILM because the posterior hyaloid was not detached
The patient denied a history of activities such as Valsalva manoeuvres that could have precipitated the hemorrhage. A comprehensive workup was performed, including a complete blood count with peripheral blood smear, serum homocysteine levels, and serological tests for systemic infections such as syphilis and HIV, all yielding normal results. Given the sudden onset of the premacular hemorrhage and the absence of a clear causal factor, a clinical diagnosis of suspected Valsalva Retinopathy (VR) was established. Optical coherence tomography (OCT) confirmed the location of the hemorrhage to be beneath the ILM, as the posterior hyaloid was not detached (Fig. 1b).
The patient was presented with various treatment options, including observation, YAG laser membranotomy, and PPV. After a thorough discussion of the potential benefits and risks associated with each option, the patient opted for YAG laser membranotomy. During the initial procedure, two laser shots at 2.5 mJ were directed to the lower edge of the hemorrhage, resulting in the blood shifting to the inferior subhyaloid space and creating a classic boat-shaped hemorrhage, which expanded gradually over the following hour (Fig. 2a-c). A follow-up consultation led to a second session of YAG laser membranotomy, delivering laser energy at a power of 5 mJ to two separate areas of the subhyaloid blood. This successfully facilitated drainage of the blood into the vitreous cavity (Fig. 2d-f).
Fig. 2
Sequential colour fundus photographs and optical coherence tomography scans after YAG laser membranotomy: a-c: Sequential color fundus photographs of the left eye taken immediately after and one hour following the delivery of two 2.5 mJ laser pulses to the inferior margin of the hemorrhage passing through the posterior hyaloid and ILM. This intervention resulted in a downward displacement of the blood into the inferior subhyaloid space, forming a classic boat-shaped hemorrhage. The accompanying optical coherence tomography images reveal that the clotted blood obstructed the potential hyaloid opening, preventing the hemorrhage from evacuating into the vitreous cavity. d-f: Following this, a second YAG laser membranotomy was performed, applying 5 mJ at two distinct locations on the subhyaloid blood. This procedure successfully facilitated the drainage of the hemorrhage into the vitreous cavity
Two days post-procedure, the patient reported a marginal improvement in visual acuity, reaching 6/96, but he also experienced a dense central scotoma attributed to thick, coagulated red blood present in front of the fovea. Consequently, PPV was recommended and performed the following day. A 25-gauge vitrectomy was conducted, which involved posterior cortical vitreous separation utilizing intravitreal triamcinolone acetonide, ILM removal facilitated by Brilliant Blue G staining, and removal of clotted sub-ILM blood using a flute needle and vitrectomy cutter (Fig. 3a-e).
On the first postoperative day, examination revealed clearance of the preretinal blood over the macula. An OCT scan demonstrated a normal foveal contour, with the ILM exhibiting a lifted edge at the junction of the peeled and non-peeled areas (Fig. 4a and b). By postoperative day 3, the premacular hemorrhage and retinal hemorrhages had resolved significantly. The visual acuity in the left eye had improved to 6/8 (Fig. 4c). The patient was advised to continue taking post-operative medications and was scheduled for a four-week follow-up examination.
Fig. 3
Intraoperative photographs depicting the surgical steps for evacuating the sub-internal limiting membrane (ILM) blood: a-e: After a 25-gauge pars plana core vitrectomy was performed, posterior cortical vitreous separation was initiated with intravitreal triamcinolone acetonide (a), ILM removal was performed following staining with Brilliant Blue G (b-d), and clotted sub-ILM blood was removed with a flute needle and vitrectomy cutter (e)
Fig. 4
Post-operative colour fundus photographs and optical coherence tomography scan after pars plana vitrectomy: a, b: On the post-operative day one visit, the preretinal blood in front of the macula had cleared, and an optical coherence tomography scan revealed a normal foveal contour with a lifted edge of the ILM (yellow arrow) at the junction of the peeled and non-peeled ILM at the macula. c: By post-operative day 3, the premacular hemorrhage and the remaining retinal hemorrhages had completely cleared and the visual acuity in the left eye had improved to 6/8
留言 (0)