
記住我





Our study included 129 patients with a mean age of 36 ± 23 years (range 1–77 years), of whom 81 (62.8%) were male. Approximately 52% of patients experienced injuries to the right eye (OD), while 48% had injuries to the left eye (OS). In terms of systemic disease history, the majority of individuals (83.7%) had no history of systemic diseases. A history of eye disease was noted in 13 patients (10.1%), and 51.2% of the patients were from rural areas (Table 1).
Table 1 Baseline demographic and clinical characteristics of study participantsThe mean length of hospital stay for patients was 2.1 ± 1.7 days, ranging from 0 to 8 days. Upon admission, patients had a BCVA of 1.29 ± 1.19 LogMAR (range 0 to 3.1), which increased to 2.06 ± 1.10 LogMAR (range 0 to 3.1) by the day of discharge. The mean time from trauma to hospital admission was 3.85 ± 0.97 h, ranging from 1 min to 36 h. For patients undergoing surgery, the mean time between admission and the first surgery was 7.48 ± 9.5 h, ranging from 15 min to 85.5 h. The mean time between the first and second surgeries for patients was 55.4 ± 90.9 days, ranging from 2 to 365 days.
In analyzing injuries to the orbital and periorbital areas, out of 129 patients, 68 (52.7%) had no specific injuries in these areas, 30 (23.3%) had eyelid lacerations, 22 (17.1%) had canalicular lacerations, 6 (4.7%) had orbital wall fractures, 1 (0.8%) had eyelid laceration with retrobulbar hemorrhage, 1 (0.8%) had mucormycosis, and 1 (0.8%) experienced simultaneous canalicular laceration and orbital wall fracture.
Seventy patients (54.3%) had open globe injuries, and 7 (5.4%) were diagnosed with endophthalmitis during hospitalization. Seventy-eight patients (60.5%) did not require intravenous antibiotics during treatment. The OTS in the study ranged from 37 to 100, with a mean score of 72.08 ± 20.78. For the 11 patients (children under 4 years) who could not respond to VA measurements, OTS could not be evaluated. Other clinical characteristics of patients are presented in Table 2 (Table 2).
Table 2 The characteristics of ocular injuries in study participantsForty-nine patients (38.3%) underwent primary repair initially. The lacrimal canalicular repair was performed on 22 patients (17.2%). Additionally, only 23 patients required more than one surgical intervention, with 11 (8.5%) undergoing lensectomy. Due to severe soft tissue damage in a patient with concurrent canalicular laceration and orbital wall fracture, lacrimal drainage system intubation was not possible in this patient (Table 3).
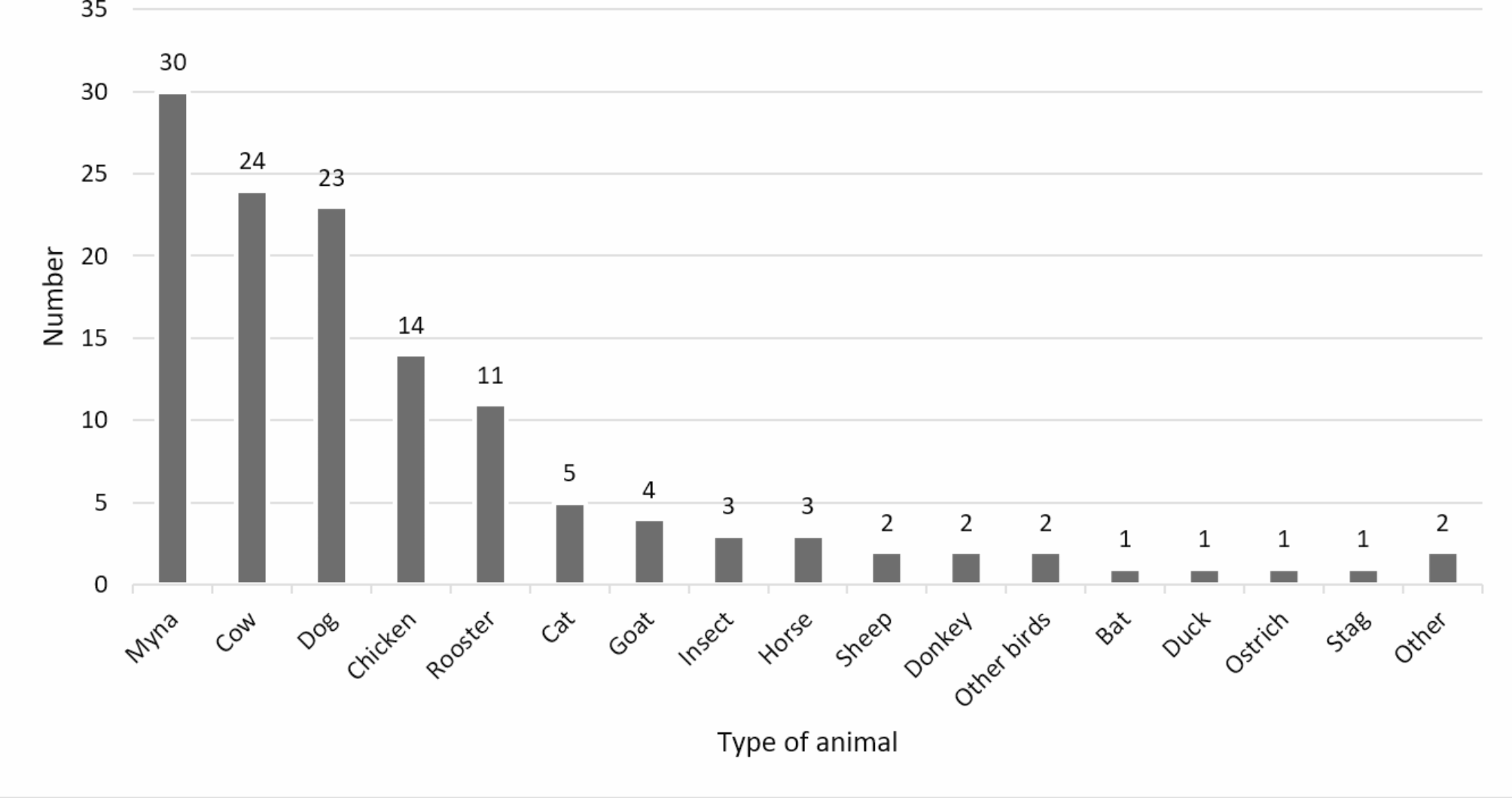
Table 3 Surgical interventions performed on study participantsIn our study, the myna was found to be the most common animal and bird causing injury, accounting for 30 patients (23.3%). Of the seven patients who developed endophthalmitis, four were injured by mynas, two by roosters, and one by a goat. Additional details regarding the types of animals and birds causing trauma can be found in Fig. 1 (Fig. 1).
Fig. 1
Descriptive data of invasive animals and birds in patients with ocular injuries
Our analysis of the type of animal and bird causing the injury and the occurrence of open globe injury shows that out of a total of 60 injuries involving birds, 47 patients (78.3%) were diagnosed with open globe injury, while this rate was 21 out of 66 (31.8%) in injuries involving quadrupeds. The difference between the two groups was statistically significant (P-value < 0.001). However, the age and gender of the patients were not significant factors in the incidence of open globe injury (P-value = 0.280 and 0.320, respectively).
Of the seven patients with endophthalmitis, six resided in urban areas, though this variance was not statistically significant (P-value = 0.058). The analysis indicated that the mean time from injury to hospital admission was 31.46 ± 3.58 h in the rural group and 29.85 ± 6.48 h in the urban group (P-value = 0.012). The time from admission to the first surgical intervention was 11.14 ± 8.8 h in the rural group and 6.83 ± 6.13 h in the urban group (P-value = 0.020).
Patients who developed endophthalmitis had a higher average time from trauma to hospital admission compared to those without endophthalmitis (70.15 vs. 24.7 h, P-value = 0.22), although this difference was not statistically significant. The duration from hospitalization to surgery was shorter in the endophthalmitis group compared to the non-endophthalmitis group, but this difference was not statistically significant (7.41 vs. 9.13 h, P-value = 0.84). The total time from trauma to surgery in patients with endophthalmitis was higher than in those without endophthalmitis (77.57 vs. 35.01 h, P-value = 0.26), but this discrepancy was not statistically significant.
Of the seven cases of endophthalmitis, six occurred in patients with Zone 1 trauma, and one occurred in Zone 3. Gender was not found to be a determining factor affecting the zone of open globe injury (P-value = 0.596). Six cases of endophthalmitis were linked to bird trauma, while one case was linked to quadruped trauma. All seven patients with endophthalmitis had a history of receiving intravenous antibiotics. The occurrence of endophthalmitis in the affected zones and the type of animals and birds involved did not show a statistically significant difference (P-value = 0.310 and 0.532, respectively). However, there was a significant difference in the incidence of endophthalmitis between the group that received intravenous antibiotics (13.7%) and the group that did not (0%, P-value = 0.027). The results of our analysis showed that with increasing age, the time interval between the occurrence of trauma and the visit to the hospital increased, although this relationship was not statistically significant (Z = 0.587, P-value = 0.557).
The BCVA at the time of admission was significantly better for urban patients (0.98 ± 1.00 LogMAR) than for rural patients (1.60 ± 1.28 LogMAR; P-value = 0.008). Similarly, at discharge, urban patients had significantly better BCVA (1.43 ± 1.11 LogMAR) compared to rural patients (2.44 ± 0.91 LogMAR; P-value = 0.002). Furthermore, patients with Zone 3 injuries had worse BCVA compared to those with Zone 1 and Zone 2 injuries, both at the time of admission (P-value < 0.001) and discharge (P-value < 0.001) (Fig. 2).
Fig. 2
Visual acuity of patients at the time of admission and discharge based on the injured zones in open globe injuries
The effects of factors such as age, time from trauma to hospital admission, and time from admission to the first surgical intervention on patients’ BCVA at discharge are summarized in Table 4. The results indicate that age has a statistically significant correlation with BCVA at discharge (correlation coefficient = 0.359, P-value = 0.015) (Table 4).
Table 4 Correlation between age, time of referral, and surgery with visual acuity during dischargeBCVA at discharge was significantly worse in patients with injuries from quadrupeds (2.80 ± 0.57 LogMAR) compared to those with injuries from birds (1.37 ± 1.04 LogMAR; P-value < 0.001). Also, our analysis revealed that a lower OTS is significantly correlated with worse BCVA at discharge (P-value = 0.031). Furthermore, the group that received intravenous antibiotics had worse visual acuity compared to the group that did not receive intravenous antibiotics (2.33 ± 0.85 and 1.31 ± 1.66 LogMAR, respectively), although this difference was not statistically significant (P-value = 0.157).
The analysis excluded LP and NLP patients, resulting in no significant differences in the BCVA at discharge compared to pre-treatment measurements (P-value = 0.686). Nonparametric correlations indicated a lack of correlation between BCVA at discharge and factors including age, time to referral, and surgery (P-value = 0.415, 0.949, and 0.397, respectively) (Table 5). Zone-based and animal category analysis revealed no significant changes in BCVA at discharge (P-value = 0.352 and 0.334, respectively). We noted no statistically significant differences in BCVA at discharge between individuals receiving intravenous antibiotics and those who did not (P-value = 0.085). The location of residence did not significantly affect the BCVA at discharge (P-value = 0.252), although rural patients experienced longer referral delays (P-value = 0.029).
Table 5 Correlation between age, time of referral, and surgery with visual acuity during discharge (after excluding patients with LP and NLP)One unique patient included a one-year-old child who experienced penetrating injury with a rooster. The child had fever, lethargy, and swelling of the eyelids seven days following primary repair. Even after receiving systemic antifungal treatment with a diagnosis of mucormycosis, the infection did not improve. Consequently, exenteration was performed.
留言 (0)