Since the issuance of government guidelines, awareness regarding ROP has increased, leading to a greater number of conducted ROP studies. A reduction in neonatal mortality has led to an increased population of babies at risk of ROP due to improvements in neonatal care. The reported rate of infants requiring treatment for ROP in our country ranges from 7.1 to 16.6% [6, 7, 10], whereas in developed countries, it ranges from 5.2 to 15.4% [16,17,18]. In Egypt, Aziz et al. reported that 12.4% of eyes exhibited high-risk ROP and required treatment [19]. A retrospective study conducted in 2022 on premature neonates from northern Iran yielded similar results [20], with the incidence of ROP requiring treatment estimated at approximately 13.4%. The result of our study was notably higher at 27.9%, surpassing most previous reports in our country. This discrepancy might be attributed to the fact that we exclusively included tertiary referral centers, which typically receive a larger number of referred patients, thereby resulting in an increased rate of ROP treatment. The percentage of ROP cases requiring treatment in this study was higher than that in other countries. This variation could be due to combined differences in neonatal care, distinct screening criteria, economic conditions, ethnicities, and other associated risk factors.
The mean GA and BW of ROP cases in this study were found to be similar to those reported in previous studies. However, the mean GA and BW in the ROP treatment group were lower than what has been previously documented [6, 10]. In this study, over half of the ROP requiring treatment had a GA of less than 30 weeks (82.6%) and a BW of less than 1250 g (73.2%). These proportions are higher than the 63.4% and 48.7% observed in a 2013 study [11]. A recent study conducted by Yang et al. also reported outcomes similar to those in our study [10]. The proportion of ROP requiring treatment occurring in infants with low GA and BW has increased, which may be associated with the improvement in medical care for neonates in China over the past few decades [21]. The workload of pediatric ophthalmologists for screening ROP is particularly burdensome due to the large population base in China. While numerous studies have confirmed the effectiveness of current guidelines, expansive screening standards seem to strain the healthcare system and lead to many unnecessary examinations. Fundoscopy for ROP screening has proven to be uncomfortable, especially for preterm babies [22]. A prospective study based in neonatal units across two tertiary-level hospitals in Shanghai indicates that by progressively narrowing the scope of screening, more cases of ROP would go undetected. However, the majority of these cases represent mild ROP that does not require treatment. It is suggested to optimize the screening criteria to include infants with a GA of ≤ 33 weeks and a BW of ≤ 1750 g, which could result in a 43% reduction in examinations [11]. Research findings from 2020 demonstrate that using an optimized model (GA < 32 weeks or BW < 1600 g) could spare examination for 2422 infants (43.2%), with only one case of Stage 1 ROP being missed (sensitivity of 98.41%) [10] A study from Hebei province proposed further narrowing the screening criteria to < 32 weeks of GA and < 1800 g of BW, resulting in a 21.6% reduction in screenings without missing severe cases [12]. Our study proposes an optimally refined screening standard of ≤ 30 weeks of GA and ≤ 1600 g of BW, which is narrower than those previously suggested in the literature.
In the internal validity verification, we observed that the sensitivity of the proposed optimized model (99.4%) is equally high compared to the sensitivity of the current screening standards, resulting in a reduction of 857 infant examination (18.0%). Although the optimized screening model may miss 8 cases, all of which are high-risk patients, these cases would also be missed by the existing screening criteria if relying solely on GA and BW. Among these 8 missed cases, 2 were Type 1 ROP, 5 were Stage 4 ROP, and 1 was Stage 5 ROP. All these patients underwent hyperbaric oxygen therapy. Among the 5 patients with Stage 4 ROP, 3 had concurrent cardiovascular diseases, and 2 had respiratory diseases. The patients with Stage 5 ROP also had a respiratory condition. Both cases of Type 1 ROP had cardiovascular diseases. However, according to the third criterion of the existing standards, which states that infants with an unstable clinical course should still be included in the screening, these 8 patients would not been missed since they present systemic high-risk factors.
The existing screening guidelines primarily rely on GA and BW. Although they demonstrate a high sensitivity in predicting severe ROP, it is crucial to acknowledge that their sensitivity is not 100%, as certain cases with higher GA and BW might also necessitate treatment. An ideal screening standard should minimize the number of screenings while ensuring that no sever ROP cases are missed. Therefore, it is essential to integrate “extra criteria” into ROP screening to improve both sensitivity and specificity. These criteria could include overall health condition and duration of oxygen therapy, and should be further refined based on high-risk factors specific in the Chinese population.
Developed countries have made significant advancements in the research of ROP screening models. In 2006, Sweden introduced the WINROP model [23], which was pioneering in incorporating postnatal factors such as Insulin-like Growth Factor 1 levels and postnatal weight gain into the ROP risk predictior. This significantly enhanced the sensitivity and specificity of screenings. Subsequently, new predictive models like the PINTROP [24], CHOPROP [25], and ROP Score models [26] were developed based on postnatal weight gain indicators. However, these models have showed inconsistent predictive performance and limited clinical utility during external validation across various countries, which has restricted their widespread application. In 2018, the United States introduced the G-ROP model [27], which was subjected to validation studies in multiple countries due to its scientific rigor, transparency, and practicality [28]. This model has been validated in developed regions like Japan and Taiwan, while its applicability might not be suitable for our country [29, 30]. Moreover, China’s research into ROP risk prediction models is still in its nascent stages. Further research should focus on conducting more in-depth prospective, multicenter studies to advance this field effectively.
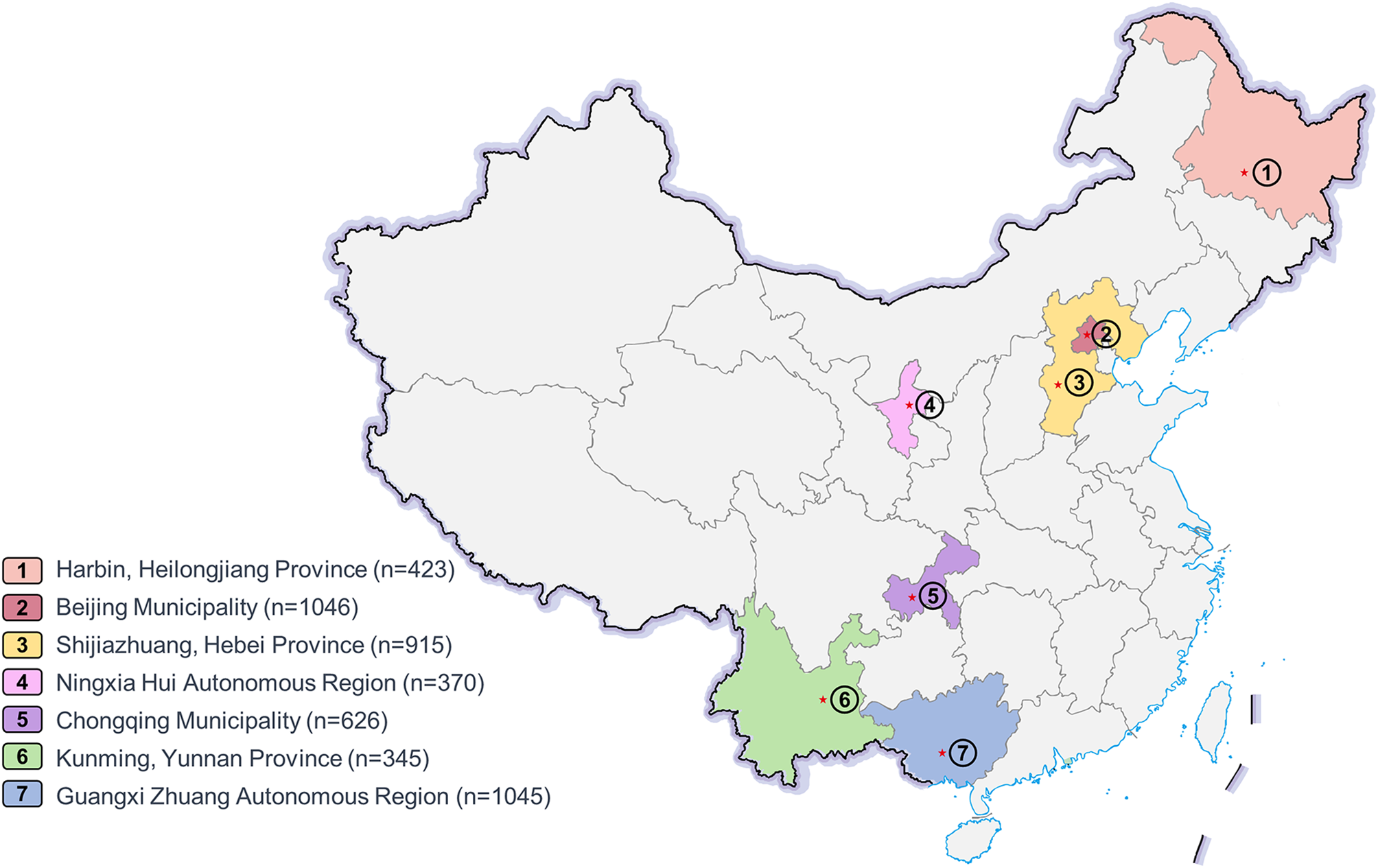
This study represents the most extensive multicenter investigation conducted to date, encompassing a wide range of geographical regions in China. However, there are additional potential limitations to consider. The first limitation was the study design. Retrospective data collection can introduce bias into the study design. The loss of patients during follow-up in the retrospective cohort study resulted in data missingness, introducing potential bias into the analysis. Second, although this study encompasses diverse regions, it cannot be considered representative of entire Chinese population. As there are variations in demographic characteristics, economic level, and healthcare conditions across different regions in china, further population-based studies on premature infants in the broader community are essential.






留言 (0)