Study population
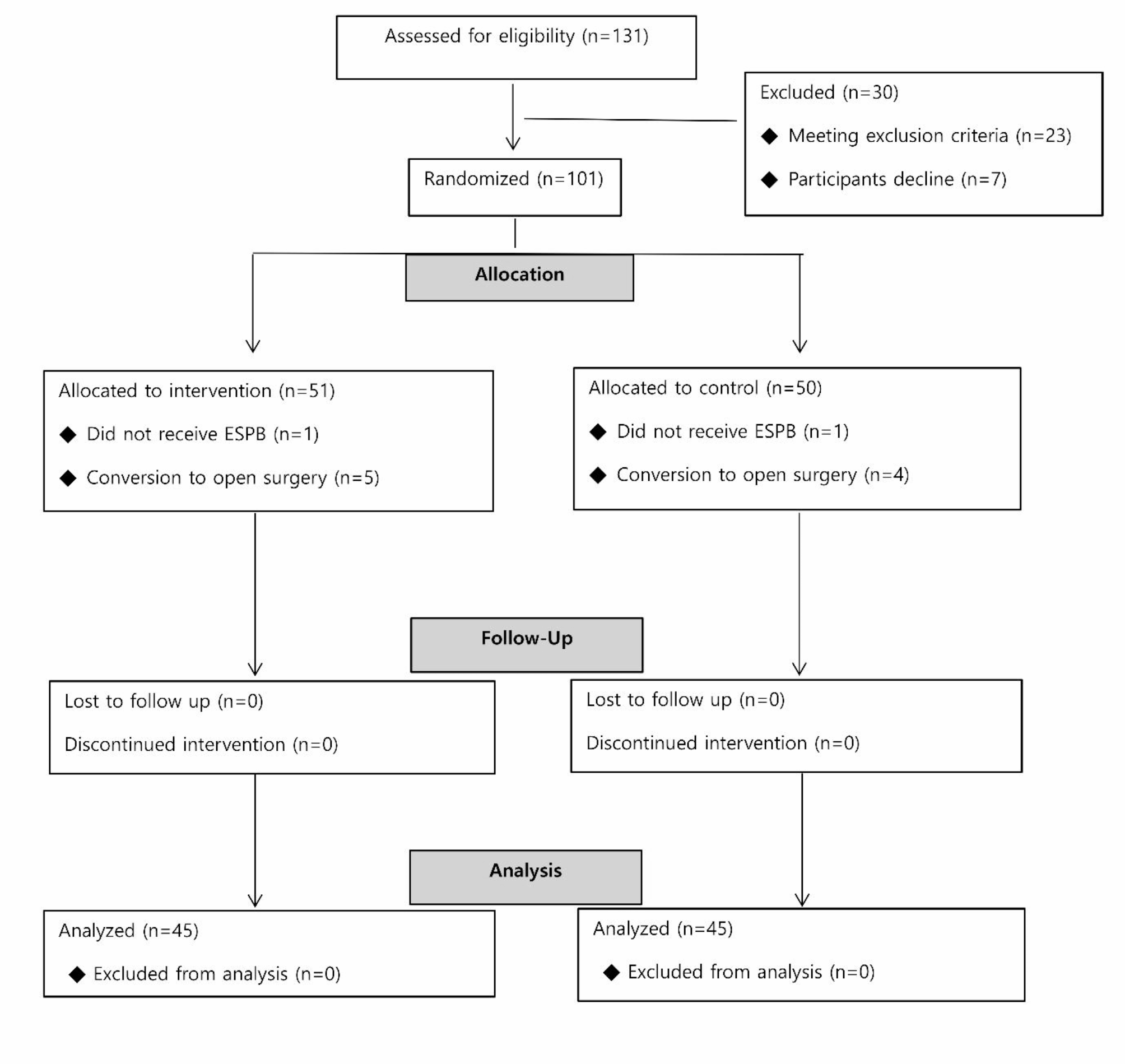
Present study was designed as a monocentric, double-blind, randomized controlled trial. The study protocol was approved by the Ethics Committee of Wonju Severance Christian Hospital (CR122093). The participants are listed at https://cris.nih.go.kr (accessed at KCT0008710; registration date: 17/08/2023). Present study was conducted in a tertiary university hospital in Wonju, Republic of Korea. Informed consent was obtained from all patients or their legal guardians before their participation. A total of 101 patients aged 19–80 years with an American Society of Anesthesiologists physical status of class 1–4 who had undergone VATS between March 2023 and September 2023 were enrolled in this study. Patients were excluded if they met at least one of the following criteria: cognitive impairment, P2Y12 inhibitor (e.g. clopidogrel, ticlopidine, ticagrelor, etc.) or anticoagulants (e.g. apixaban, dabigatran, edoxaban, rivaroxaban, warfarin, etc.) administration within the 48 h, taking dual anti-platelet drug defined as combination of aspirin and a P2Y12 inhibitor, infection at the surgical site, patient refusal, pregnancy, allergy to ropivacaine, sepsis, anatomical deformity of the thorax, and increased intracranial pressure.
Randomization and blinding
The participants were randomized and allocated to paracetamol or saline group using a computerized randomization table. A random allocation sequence was generated at 1:1 ratio by an anesthetist who was not involved study using a computer-generated table of random numbers sealed in opaque envelopes. Each envelope was opened by one of the authors (S.K.), and notified the group allocation to a nurse in preparation room immediately before surgery. Paracetamol (1 g with saline 100 mL) or saline (100 mL) were administered during the surgery. Patients and the investigator (H.L.) involved in the postoperative data collection were maintained blinding during the observational period. Therefore, design of the present study was double-blind.
Perioperative management
No premedication was given before the induction of anesthesia. On arrival in the operating room, patients were monitored with 3-lead electrocardiogra, pulse oximetry, noninvasive blood pressure, and Sedline® electroencephalography guidance (Masimo, Irvine, CA, USA). A bolus of propofol (1.5–2 mg/kg), remifentanil (1 µg/kg) and rocuronium (0.6 mg/kg) were used to induce anesthesia. Patients were intubated with a double-lumen endobronchial tube (DLT, Blue Line®, Smith Medical US, Minneapolis, 37Fr for men and 35 Fr for women) and arterial catheterization was performed. Anesthesia was maintained by administration 1.5-2.5% of sevoflurane or 4.0–6.0% of desflurane, 0.05–0.3 µg·kg− 1·min− 1 of remifentanil and 0.3 to 0.6 mg·kg− 1·min− 1 of rocuronium.The infusion rate of remifentanil was adjusted according to the overall hemodynamic data by the attending anesthesiologist, who also suggested the intensity of the surgical stimuli. The infusion rate of rocuronium was adjusted using a Train of Four watch value was less than 2. Inhalational anesthetics were administered as fractions under Sedline® value was 25 to 50. Acetphen premix® (HK Innoen Inc., Korea) or saline (100 mL) were administered intravenously over a 15-min at the end of the surgery in the paracetamol and control groups, respectively. ESPB was performed subsequently with the patient in the lateral position. The analgesic blocks were performed by the same anesthesiologist (S.K.). Fentanyl (18 mcg/kg) and ramosetron (0.3 mg) were dispensed via intravenous patient-controlled analgesia. The fentanyl dose was recorded as morphine milligram equivalents (MME). The patients were transported to the postanesthetic care unit (PACU) or surgical intensive care unit (ICU) following extubation in the operating room. Nefopam (20 mg) and fentanyl (50 ug) were administered intravenously to patients with visual analog scale (VAS) scores of 4–6 and > 6 in the PACU, respectively, according to the standard analgesic algorithm. The primary physician oversaw postoperative pain management after discharge of the PACU. The dosage of postoperative analgesics was recorded in MME. Intravenous tramadol (50 mg), intramuscular or subcutaneous meperidine (25 mg), oral ultracet (tramadol [37.5 mg]/acetaminophen [325 mg]), and transdermal fentanyl patches (25 mcg/h) were used postoperatively. Withdrawal from the study was considered in case of conversion to the open surgery, hypersensitivity reaction during anesthetic induction.
Surgical techniques and intercostal nerve block
The surgeon (C.S.B.) performed the conventional three-port VATS technique by making a utility incision 3–4 cm in size at the T4 level. Posterior instrument and camera ports 1 cm in size were placed at the T7 and T8 levels, respectively. Nerve-sparing techniques were not used. At the end of the surgical procedure, intercostal nerve block was performed from the T4–T9 levels using 2 mL of 0.375% ropivacaine for each level.
Erector spinae plane block
ESPB was performed by injecting 20 mL of 0.375% ropivacaine into the fascial plane between the tips of the transverse process and erector spinae muscle at the T5 level under ultrasound guidance. A 21-guage ultrasound-visible needle (Echoplex; Vygon, Ecouen, France) was inserted in the craniocaudal direction. The position of the needle tip was confirmed via hydro-dissection with 2–3 mL of saline, and the anesthesiologist aspirated every 5 mL to prevent intravascular injection.
Outcome measures
The primary outcome measure of the present study was the analgesic efficacy of adjuvant paracetamol after VATS with ESPB. The VAS pain score was measured in the PACU as well as 6, 12, 24, and 48 h postoperatively. The highest VAS scores were recorded at each timepoint. The secondary outcome measures included the total dose of analgesics administered to patients (in MME), satisfaction score, length of hospital stay, perioperative liver enzyme (AST, ALT) and incidence of nausea and vomiting.
Sample size calculation
The sample size was calculated based on the previous numeric rating scale (NRS) pain scores. The mean pain score after VATS with ESPB in a previous study was 5.96 ± 1.68 [10]. The number of patients enrolled in each group was estimated to be 45 if the administration of paracetamol enhanced the pain score by ≥ 1.0 points (type I error, 0.05; power, 0.90). Fifty patients were enrolled in each group, considering a dropout rate of 10%.
Statistical analysis
All statistical analyses were performed using IBM SPSS (IBM SPSS Statistics for Windows, version 25; IBM Corporation, Armonk, NY, USA). The Shapiro–Wilk test was used to assess the distribution of continuous variables. Independent t-test and the Mann–Whitney U test were used to analyze outcome variables with and without a normal distribution, respectively. The data are presented as the mean and standard deviation for normally distributed data and as median and interquartile range for non-normally distributed data. The Chi-square test was used to analyze the frequency. Repeated-measures analysis of pain scores was performed with a post-hoc Bonferroni correction.


留言 (0)