Patients
Patients aged 60 to 85 years, with an American Society of Anesthesiologists (ASA) physical status of I-III, a Body Mass Index (BMI) between 18 and 30 kg/m² and stones from 4 mm to 15 mm who were undergoing elective UHLL, were recruited for this randomized controlled trial. The exclusion criteria included impacted stones, sepsis, sleep apnea syndrome, asthma, severe respiratory insufficiency, a history of COVID-19 infection, recent myocardial infarction, uncontrolled hypertension, high-risk coronary artery disease, severe hepatic and renal insufficiency, and gastroesophageal reflux.
Randomization and blinding
Randomization (1:1 ratio, with block sizes of 2 and 4, stratified by sex) was performed using the Sealed Envelope online randomization tool (https://www.sealedenvelope.com/simple-randomiser/v1/lists). The randomization was stratified by gender, considering that female patients tend to experience poorer postoperative recovery. The resulting random allocations were enclosed within sequentially numbered opaque envelopes and sealed before surgery began. After the induction of anesthesia, an independent researcher, who was unaware of the randomization process, unveiled the envelopes and assigned patients to either the HFNC group or the laryngeal mask airway (LMA) group. The anesthesiologists responsible for patient care were informed of the study medications and anesthesia method, while the surgeons and other members of the healthcare team remained uninformed. The subjects, clinicians (excluding the anesthesiologists), and investigators involved in patient recruitment and outcome assessment were completely blinded to the group assignments. The two assessors did not access anesthesia records and were not involved in direct patient care.
Anesthesia and study interventions
Baseline HR, arterial blood pressure (via radial artery cannulation), 3-lead electrocardiography (ECG), peripheral oxygen saturation (SpO₂), and bispectral index (BIS; Medtronic, Minneapolis, MN, USA) were monitored throughout the procedure. After the subjects were situated in the operating room, a single 10 ml dose of 2% lidocaine was administered and retained in the urethra for 10–15 min.
In the LMA group, general anesthesia was induced using i.v. propofol 1–2 mg/kg and fentanyl citrate 0.5–1.5 µg/kg. Neuromuscular blockade was achieved with cisatracurium benzoate 0.15 mg/kg for laryngeal mask placement. After laryngeal mask placement, the mechanical ventilation was set the IPPV(Intermittent Positive Pressure Ventilation) mode, and the parameters were tidal volume of 6 to 8 ml/kg, appropriate positive end-expiratory pressure, and a respiratory frequency of 12–16 breaths/min. A normal end-tidal carbon dioxide (CO2) tension (35 to 45mmHg) was maintained by adjusting the respiratory frequency and the tidal volume intraoperatively. Anesthesia was maintained using remifentanil hydrochloride 0.1–0.3 µg/kg/min and propofol 3–5 mg/kg/h, with adjustments to maintain BIS values between 40 and 60. During surgery, cisatracurium 0.03 mg/kg bolus injections were administered as needed for neuromuscular blockade. After surgery, the patients would get reversal agents according to the anesthetist’s decision.
In the HFNC group, general anesthesia was induced using i.v. fentanyl 0.5–1.5 µg/kg and propofol 1–2 mg/kg. Anesthesia was maintained at the targeted depth (BIS 50–80) by manually adjusting i.v. propofol 1–2 mg/kg/h and remifentanil 0.1–0.3 µg/kg/min. No neuromuscular blockers were used, allowing subjects in the HFNC group to maintain spontaneous breathing. Oxygen was provided via high-flow nasal cannula (HFNC) with humidified oxygen therapy [30.0 L/min; FiO₂, 100%; and gas temperature, 37.0 °C]. If the pulse oxygen level fell below 93%, the attending anesthesiologists increased the oxygen flow to maintain normal oxygenation. Tracheal intubation could be considered if necessary for safety. If movement occurs during the operation, a single 5 ml dose of 2% lidocaine was administered and retained in the urethra for 3 min, meanwhile additional propofol 30–50 mg was used intravenously.
For both groups, dexamethasone (5 mg) and ondansetron (4 mg) were administered to prevent postoperative nausea and vomiting (PONV). Patients experiencing intraoperative blood pressure below 80% of the baseline value were administered intravenous ephedrine (5 mg), phenylephrine (40 µg), or underwent rapid fluid replacement. After surgery, patients were transferred to the Post-Anesthesia Care Unit (PACU), where the level of anesthesia recovery was assessed using the Aldrete score.
Study outcomes
The primary outcome was the QoR-15 scores after surgery, as defined by the QoR-15 questionnaire [19]. This global assessment tool evaluates postoperative recovery across five dimensions: physical comfort (5 items), physical independence (2 items), emotional state (4 items), psychological support (2 items), and pain (2 items). Each item is rated on an 11-point scale, with higher scores indicating greater frequency of positive outcomes and lower frequency of negative outcomes. The overall score ranges from 0 (indicating the poorest quality of recovery) to 150 (indicating the best quality of recovery).
Secondary outcomes primarily included the length of PACU stay, time to out-of-bed mobilization, airway dryness scores [20], rate of postoperative sore throat, cough, sputum, and surgeons’ satisfaction (three surgeons have consistent professional title level, rich clinical experience and rigorous scientific research attitude). Safety outcomes were assessed, including hypoxemia (defined as a pulse oxygen level < 93% for at least 1 min), hypotension (defined as a reduction in mean arterial pressure (MAP) > 30% of the baseline value for at least 1 min), hypertension (defined as an increase in MAP > 30% of baseline for at least 1 min), bradycardia (defined as heart rate (HR) < 50 beats per minute for at least 1 min), and tachycardia (defined as HR > 100 beats per minute for at least 1 min) during surgery and in the PACU. Sedation in the PACU (defined as an Observer’s Assessment of Alertness/Sedation Scale (OAA/S) ≤ 3) and the occurrence of headache, dizziness, nightmares, or hallucinations within 0–24 h after surgery were also considered. Symptoms (nausea, vomiting, nightmares, hallucinations, and delirium) were documented during ward visits by blinded assessors. Hemodynamic events, interventions, sedation in the PACU, and the duration of PACU stay were recorded in the Surgical Anesthesia Information System (Hangzhou Zejin Information Technology Co., Ltd, Hangzhou, China). Postoperative opioid consumption, rescue analgesia, occurrences of sore throat, cough, sputum, and the length of postoperative hospital stay were documented in electronic medical records and nursing notes. 7-day follow-up data were obtained via telephone. All information was collected in the electronic case report form, which was reviewed by the principal investigator (JL) and an independent data monitoring committee.
Sample size
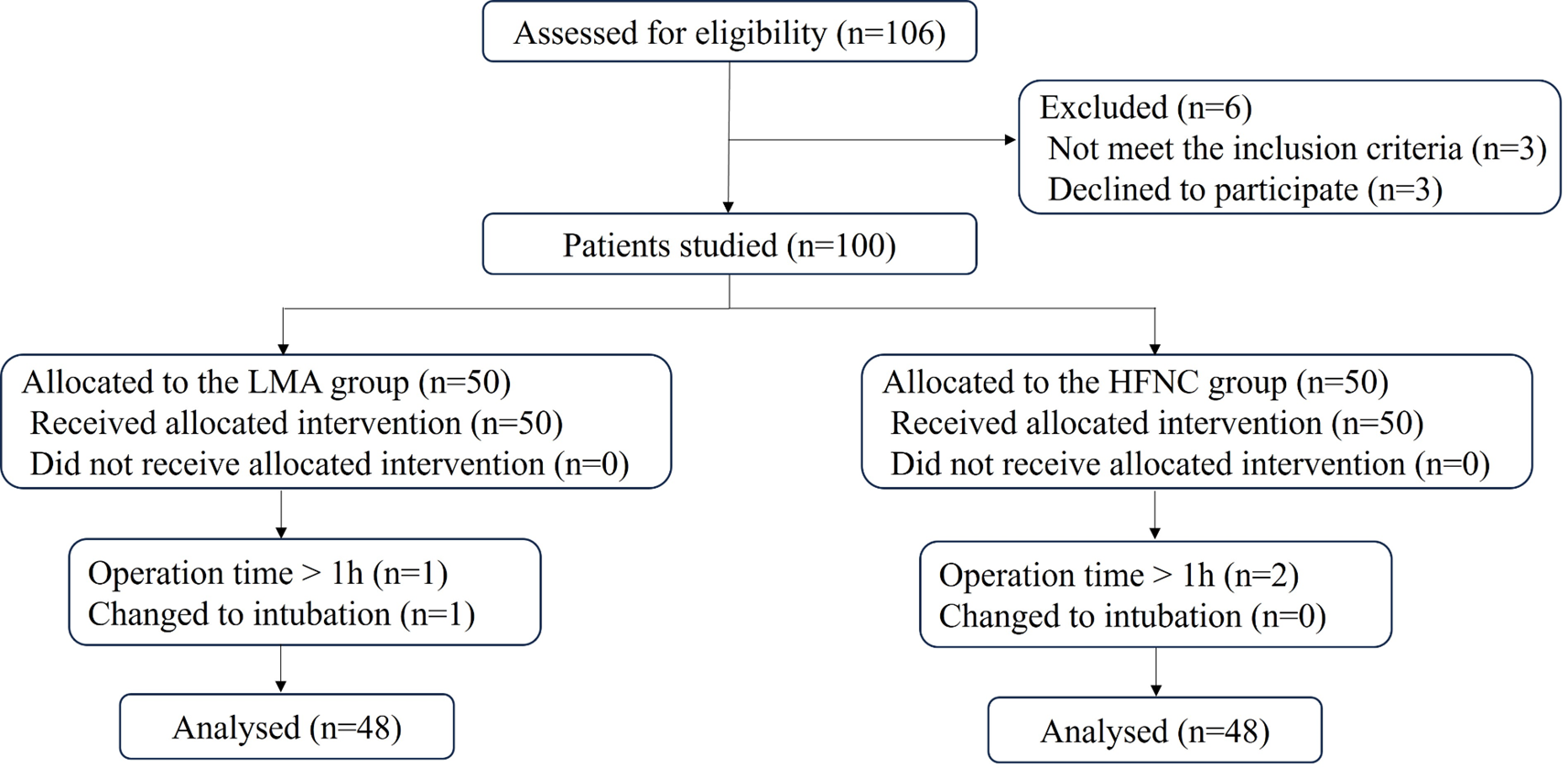
Our primary outcome was the quality of recovery (QoR-15) score 24 h post-surgery. The minimum clinically important difference (MCID) in QoR-15 score after surgery is 8 [21], and the standard deviation (SD) of QoR-15 scores (range, 1-150) is typically 10–16. We considered a difference in the mean QoR-15 scores between groups of 8 as clinically significant. We selected an SD of 13 to best reflect our study population. Assuming a two-sided α of 0.05 and a power of 80%, sample sizes were calculated using PASS 15 software, resulting in N1 = 43 for the LMA group and N2 = 43 for the HFNC group. Considering a possible dropout rate of 20%, a minimum of 53 subjects was required for each group, totaling at least 106 study subjects.
Statistical analysis
The assessment of data distribution was conducted using the Shapiro-Wilk test, and the results are presented as mean (standard deviation [SD]), median (interquartile range [IQR]), or number (%), as appropriate. Perioperative data and study outcomes were compared using the Mann-Whitney U test, chi-square test, or Fisher’s exact test, as deemed appropriate. The estimated effect size was reported in the form of risk difference or relative risk for binary outcomes, hazard ratio for time-to-event, and mean or median differences for continuous data with confidence interval (CI). We defined subjects with BMI > 25 as overweight. We categorized patients who had a QoR-15 score < 121 at 24 h post-surgery as having a moderate-poor quality of recovery. We divided the QoR-15 scores into poorer early postoperative recovery (QoR-15 score < 121) and better early postoperative quality of recovery (QoR-15 ≥ 121) [22]. Furthermore, prespecified subgroup analyses were performed on the primary outcome by sex (female vs. male), current smoking status (no vs. yes), and BMI scores (≤ 25 vs. > 25). For the secondary outcomes, multiple comparisons were not corrected; thus, these results should be interpreted as exploratory. Interim analysis or missing data imputation was not performed. The statistical analysis was performed using SPSS software (version 25.0, IBM SPSS Inc). A two-sided P-value of less than 0.05 was considered indicative of a statistically significant difference.


留言 (0)