
記住我

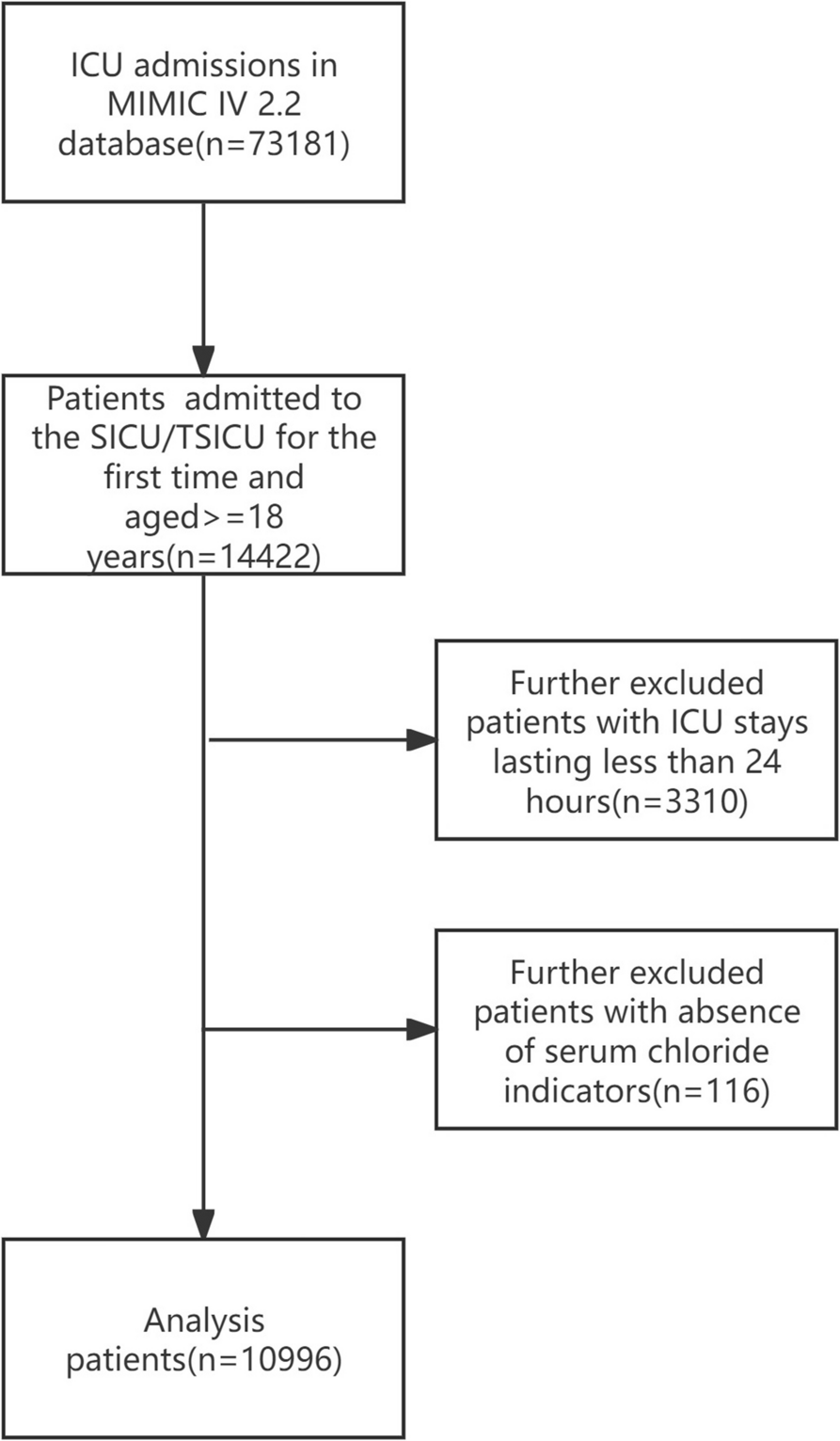
This study encompassed 10,996 patients admitted to the SICU, with 54.43% (n = 5984) identified as male and 45.58% (n = 5012) as female. The median age was 63 years (IQR 51–76). Table 1 displays the baseline characteristics of the patients. Serum chloride levels were segmented into four quartiles: Q1 (61–101 mmol/L), Q2 (101–104 mmol/L), Q3 (104–108 mmol/L), and Q4 (108–140 mmol/L). The average ICU stay was 2.58 days, and the mean hospital stay was 8.25 days. The 30-day mortality rate post-admission was 12.78%, increasing to 17.14% at 90 days and 20.32% at 180 days. Lower serum chloride levels were linked with several factors, including advanced age, myocardial infarction, heart failure, COPD, liver disease, diabetes, renal disease, AKI, APS III, elevated heart rate, increased WBC count, reduced sodium levels, elevated BUN levels, higher PT levels, use of diuretics, receipt of CRRT, need for ventilator support, prolonged hospital LOS, and increased mortality rates at 30, 90, and 180 days (p < 0.001).
Table 1 Characteristics and outcomes of participants categorized by serum chlorideClinical outcomesKaplan–Meier survival analysis curves were constructed to evaluate 30-day, 90-day, and 180-day mortality rates for patients in the SICU, grouping serum chloride levels into quartiles (Fig. 2). Marked differences in survival probabilities emerged among the four serum chloride quartiles throughout the 30-day, 90-day, and 180-day follow-up intervals (P < 0.001). Notably, within the 30-day observation period in the SICU, patients classified within the first quartile (Q1) showed the lowest survival probabilities, while those in the third quartile (Q3) exhibited the highest. This pattern persisted during the 90-day and 180-day follow-up periods.
Fig. 2
Kaplan–Meier survival analysis curves. For (A) 30-day, (B) 90-day, and (C) 180-day all-cause mortality
Employing the Cox proportional hazards model, an extensive evaluation was undertaken to assess the link between serum chloride levels and all-cause mortality among patients admitted to the SICU (Table 2). Model 4 indicated that, after adjustment for all covariates, serum chloride, analyzed as a continuous variable, was significantly associated with mortality at 30-day (HR = 0.96, 95%CI: 0.95–0.97, p < 0.001), 90-day (HR = 0.97, 95%CI: 0.96–0.98, p < 0.001), and 180-day (HR = 0.97, 95%CI: 0.96–0.98, p < 0.001) intervals. Even after serum chloride levels were divided into four groups, notable statistical differences persisted in mortality rates at 30-day, 90-day, and 180-day intervals among these groups in Model 4 (p < 0.001) (Table 2).
Table 2 Cox proportional hazard ratios for 30-day, 90-day and 180-day all-cause mortalityTable 3 Subgroup analysis of the relationship between serum chloride and 30-day, 90-day, 180-day mortalityTo probe the potential non-linear connection between serum chloride levels and clinical outcomes, the restricted cubic spline (RCS) model was utilized (Fig. 3). Following adjustment for all covariates, RCS curve analysis revealed a non-linear inverse relationship between serum chloride concentrations and mortality risks at 30 days, 90 days, and 180 days, with P-values for non-linearity recorded at 0.032, 0.002, and 0.002, respectively. Moreover, it was observed that below a concentration of 104 mmol/L, a reduction in serum chloride levels was linked with an elevated risk of mortality.
Fig. 3
Restricted cubic spline curve. Illustrating the hazard ratio for serum chloride after adjusting for Gender, Age, Weight, APSIII, OASIS, SOFA, LODS, GCS, Heart rate, SBP, DBP, Temperature, Glucose, WBC, RBC, Platelet, Calcium, Potassium, Sodium, Creatinine, BUN, PT, Myocardial infarct, Heart failure, Cerebrovascular disease, COPD, Liver disease, Diabetes, Renal disease, Malignant cancer, Hypertension, AKI, Diuretics,Ventilator, CRRT. A 30-day mortality, B 90-day mortality, C 180-day mortality
Subgroup analysisIn this study, subgroup analyses were conducted on SICU patients differentiated by age, gender, myocardial infarct, cerebrovascular disease, COPD, liver disease, diabetes, malignant cancer, and hypertension to investigate the link between serum chloride levels and all-cause mortality (Table 3). Results demonstrated a significant negative association between serum chloride levels and all-cause mortality across specific subgroups: age < 63 (HR: 0.63, 95%CI: 0.51–0.77, p < 0.001), female (HR: 0.68, 95%CI: 0.58–0.78, p < 0.001), absence of diabetes (HR: 0.74, 95%CI: 0.66–0.83, p < 0.001), and absence of hypertension (HR: 0.68, 95%CI: 0.59–0.79, p < 0.001). Further analyses indicated that the negative association between serum chloride levels and mortality was consistent regardless of the presence of myocardial infarct (YES: HR 0.72, 95% CI: 0.53–0.96, p = 0.035 vs. NO: HR 0.81, 95%CI: 0.72–0.90, p < 0.001), cerebrovascular disease (YES: HR 0.82, 95%CI: 0.69–0.97, p = 0.030 vs. NO: HR 0.73, 95% CI: 0.64–0.84, p < 0.001), COPD (YES: HR 0.77, 95%CI: 0.62–0.96, p = 0.031 vs. NO: HR 0.80, 95%CI: 0.71–0.90, p < 0.001), liver disease (YES: HR 0.59, 95%CI: 0.46–0.77, p < 0.001 vs. NO: HR 0.86, 95%CI: 0.76–0.96, p < 0.017), or malignant cancer (YES: HR 0.74, 95%CI: 0.57–0.96, p = 0.031 vs. NO: HR 0.80, 95% CI: 0.71–0.90, p < 0.001). These patterns persisted across mortality assessments at 90-day and 180-day intervals. Moreover, significant interactions were identified within age and gender groups concerning 30-day, 90-day, and 180-day mortality outcomes.
留言 (0)