
記住我

Patients aged 18 years or older diagnosed with sepsis-induced encephalopathy with septic shock were included.
➢ Sepsis was defined as suspected or evident infection and patients who had two or more quick SOFA scores: [9]
➢ Septic shock was defined as sepsis-induced hypotension that persists despite adequate fluid resuscitation and serum lactate level ≥ 2 mmol/l [10].
➢ Encephalopathy was diagnosed as GCS less than 15.
Exclusion criteriaPatient refusal, cerebral infection or known cerebral lesion, severe internal carotid artery (ICA) stenosis > 70%, pregnancy, drug intoxication, and patients supported with an intra-aortic balloon pump.
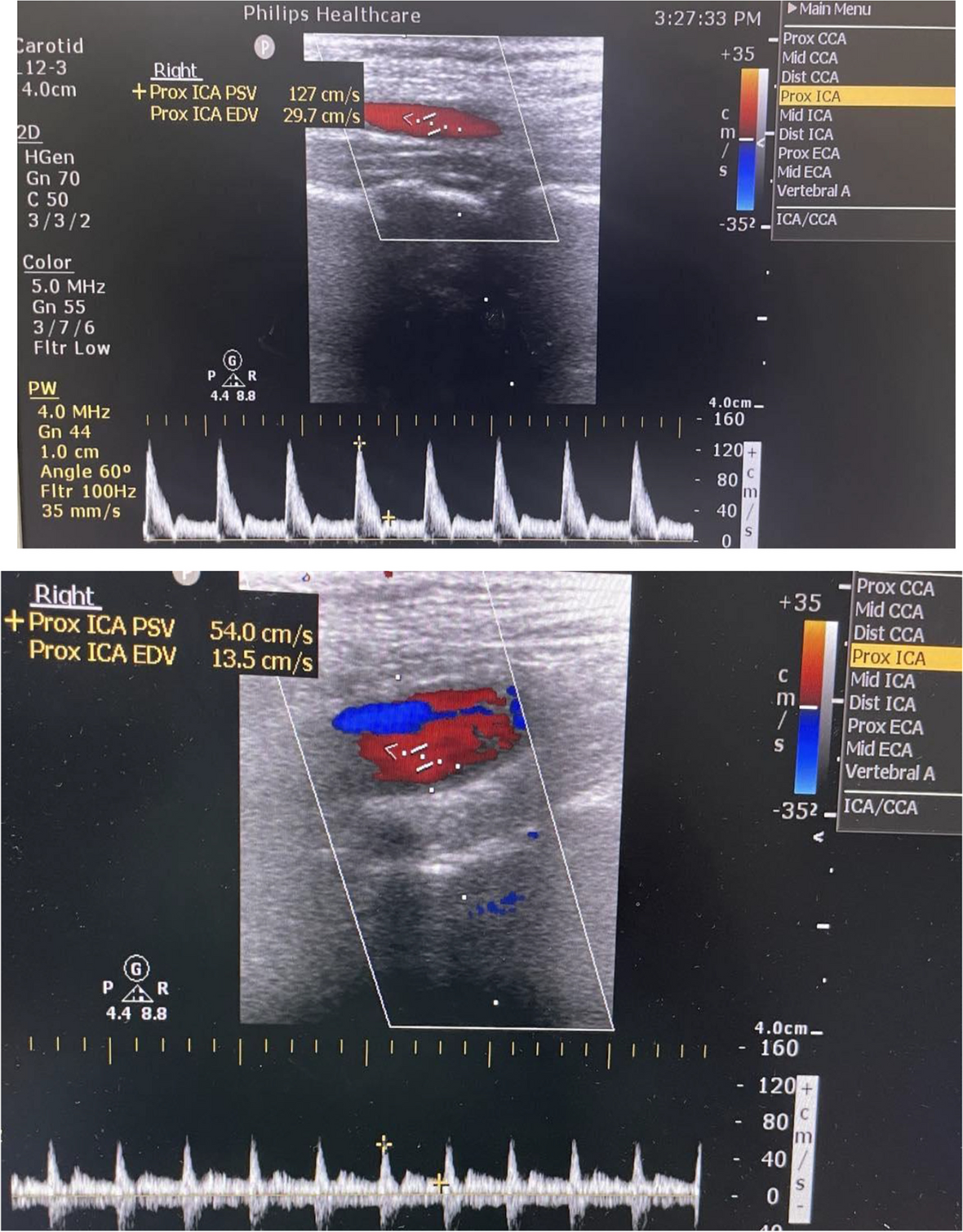
Study designPatients who met these criteria; were enrolled in this trial and were randomly and equally divided into two groups; Ultrasound assessment of the ICA and common carotid artery. (CCA) was performed to exclude cases with severe carotid artery stenosis > 70%. The criteria for diagnosis of severe ICA stenosis (> 70%) include the following: [11] PSV of ICA ≥ 215 cm/s, EDV of ICA ≥ 65 cm/s, internal to common carotid artery PSV ratio ≥ 3.7, as shown in Fig. 1.
Fig. 1
Ultrasound assessment for diagnosis of ICA stenosis showing normal ICA
All patients were managed according to the SSC guidelines for managing septic shock [12] which started within the first hour except for norepinephrine (NE) titration guided by the TCD pulsatility index in group I and the MAP in group II. Fluid resuscitation was started by administrating lactated ringer solution at a rate of 4 to 6 ml/kg.
Re-evaluation was performed after 15 min. If the MAP was still ≤ 65 mmHg, we continued resuscitation at a rate of 4 to 6 ml/kg. Re-evaluation was also performed after 15 min; until 30 ml/kg was reached. Norepinephrine was started when the patient was still hypotensive with a MAP < 65 mmHg, either during or after fluid resuscitation, even peripherally, to avoid delay until central venous access was secured. NE was the vasopressor used in this study. The norepinephrine formula used in this clinical trial was NE tartrate (ampoule preparation contains 8 mg NE tartrate, equivalent to 4 mg NE base). For patients with inadequate MAP, despite NE dose escalation up to 0.5 µg/kg/min, we added epinephrine as vasopressin wasn`t commercially available.
At the same time, the following steps were done; serum lactate measurements, obtaining appropriate routine microbiologic culture, broad-spectrum antibiotic administration, and rapid source control.
In group I, patients were placed in a supine position with the head of the bed elevated to approximately 30 to 45 degrees. Three measurements were taken, and the average value was recorded. The flow velocity of the middle cerebral arteries was measured using a low frequency 1–5 MHZ (phased-array) transcranial Doppler probe on both sides. The probe was positioned over the temporal bone window above the zygomatic arch just anterior to the patient’s ear at the level of the eye, and then a sliding motion was performed to scan through the adjacent brain tissue.
First, the temporal bone was identified, followed by the midbrain, which is butterfly-shaped, was identified. Just anterior to the midbrain, the circle of Willis was located and identified using color-coded sonography.
The middle cerebral artery (MCA) was identified as a linear, red structure as the blood flow was directed toward the ultrasound transducer. The blood flow velocity within the vessel was measured via pulsed wave (PW) Doppler.
The normal flow velocity of the MCA was associated with a steep upstroke in systole and stepwise deceleration in diastole.
The peak systolic velocity (PSV), end-diastolic velocity (EDV), and mean flow velocity (MFV) were measured. The pulsatility index (PI) was calculated by using the following equation: , as shown in Fig. 2.
Fig. 2
Measurements of pulsatility index of right MCA (PSV 127 cm/s, EDV 50.3 cm/s, MFV 75.7 cm/s, PI 1.01)
Our goal was to guide norepinephrine titration to maintain a pulsatility index below 1.3. The pulsatility index was assessed twice daily unless hypotension occurred; reassessment was performed at this time to guide NE titration.
CPP was calculated by TCD in both groups at the time of hypotensive episodes via the following equation: CPP = MAP x (EDV/MFV) + 14. [14] 14 mmHg is a calibration (zeroing) parameter established. Its normal range is 60–80 mm Hg [15].
In group II, the MAP was measured continuously, and our goal was to guide norepinephrine titration to maintain MAP ≥ 65 mmHg.
ICU mortality was the primary outcome, whereas MAP, CPP, norepinephrine titration, SOFA score, ICU stay duration, and GCS values were the secondary outcomes.
Data collectionAll registered patients were subjected to the following measurements:
The demographic data, hemodynamic parameters (MAP, heart rate), serum lactate level, SOFA score at admission and discharge, total norepinephrine dosing, duration of norepinephrine infusion, CPP, encephalopathy outcome according to GCS score, duration of ICU stay and ICU mortality.
Sample size analysisThe sample size and power analysis were calculated using the Epi-Info software statistical package created by the World Health Organization and Center for Disease Control and.
Prevention, Atlanta, Georgia, USA version 2002.
The criteria used for sample size calculation were as follows:
The expected incidence of mortality cases of sepsis-induced encephalopathy in the best intervention group is 20% compared to 45% in the least favorable intervention group.
The sample size based on the previous criteria was found at N = 56 in each group.
Statistical analysisStatistical analysis was done by SPSS v26 (IBM Inc., Chicago, IL, USA). Shapiro-Wilks test and histograms were used to evaluate the normality of the distribution of data. Quantitative parametric variables were presented as mean and standard deviation (SD) and compared between the two groups utilizing an unpaired Student’s t-test. Quantitative non-parametric data were presented as the median and interquartile range (IQR) and were analyzed by the Mann Whitney-test. Qualitative variables were presented as frequency and percentage (%) and analyzed utilizing the Chi-square test or Fisher’s exact test when appropriate. A two-tailed P value < 0.05 was considered statistically significant.
留言 (0)