Study design
This paper has been uploaded to ResearchSquare as a preprint (https://www.researchsquare.com/article/rs-4270156/v1?).
This single-center, double-blind randomized clinical trial was approved by the Clinical Trials Ethics Committee of Lishui People’s Hospital (approval no. 2023 − 137) by Chairperson Prof Zhichao Shi on 15 August 2023.This trial was performed in accordance with the Declaration of Helsinki. We followed the Consolidated Standards of Reporting Trials reporting guidelines, and all enrolled patients provided written informed consent.
Inclusion and exclusion criteria
This study involved 86 adult patients who were admitted to Lishui People’s Hospital for nasal surgery from September 2023 to October 2023.
The inclusion criteria were (1) elective nasal surgery, (2) aged 18–65 years, (3) American Society of Anesthesiologists physical status of I or II, and (4) body mass index of 18.5–27.9 kg m− 2. The exclusion criteria were (1) preoperative mental disorders or communication difficulties, (2) severe arrhythmia, such as sick sinus syndrome, second- or third-degree atrioventricular block, or heart rate (HR) < 50 beats min− 1), (3) scheduled to be sent to the intensive care unit after surgery, and (4) allergy to benzodiazepines or a long-term history of benzodiazepine use.
Randomization and masking
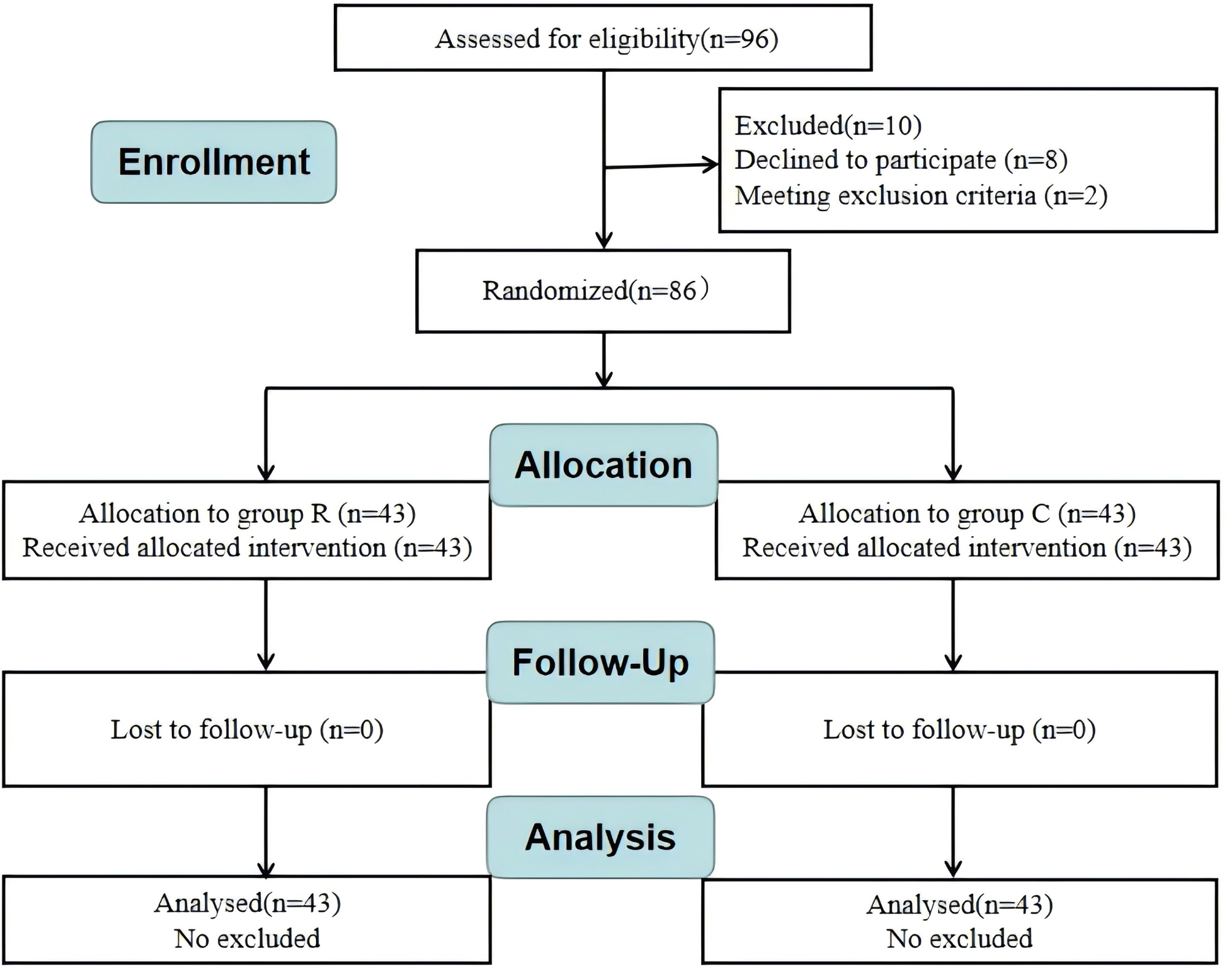
Patients were randomly assigned to two groups (Group R and Group C) using computer-generated random numbers (43 patients in each group). We discreetly kept the randomization results in envelopes until the end of the study. Study drugs were prepared by a nurse who was not involved in the other parts of the study. Both remimazolam and saline are colorless liquids, and they were digitally encoded so that the researchers who were responsible for the postoperative follow-up and data processing were blinded to the group allocation during the whole study period. All anesthetists and patients were also blinded to the group allocation.
Interventions
Patients fasted for 8 h. No premedication was administered. Upon arrival in the operating room, all patients underwent pulse oxygen saturation, mean arterial pressure (MAP), and HR measurements using a Carestation 620 A2 monitor (GE Healthcare, Chicago, IL, USA). The depth of general anesthesia of the patients was continuously monitored using a bispectral index (BIS) sensor (Canwell Medical Co., Ltd., Jinhua, Zhejiang, China). All patients were anesthetized using standard protocols as follows. Anesthesia was induced with 2.0 to 2.5 mg kg− 1 propofol (Beijing Fresenius Kabi Pharmaceutical Co., Ltd., Beijing, China), 0.4 to 0.5 µg kg− 1 sufentanil (Yichang Humanwell Pharmaceutical Co., Ltd., Yichang, China) and 0.2 mg kg− 1 cis-atracurium (Jiangsu Hengrui Pharmaceutical Co., Ltd., Jiangsu, China). After successful induction of general anesthesia, endotracheal intubation was performed. Volume-controlled mechanical ventilation was administered to maintain an end-tidal carbon dioxide partial pressure of 35–45 mmHg. Anesthesia was maintained with inhalation of a mixture of 1.5–3.5% sevoflurane (Jiangsu Hengrui Pharmaceutical Co., Ltd.) and 50% oxygen (flow rate = 2 L min− 1). The sevoflurane concentration was controlled according to the hemodynamics and BIS value of each patient (maintaining both MAP and HR to within 20% of baseline, and a BIS value of 40–60). During the surgery, sufentanil and cis-atracurium were injected as needed. When the surgery was over, the anesthetic drugs were stopped immediately. Then, the intervention measures were started, as follows. (1) Group R (n = 43): 0.1 mg/kg remimazolam was injected intravenously after surgery, and the infusion time was 1 min. (2) Group C (n = 43): 0.9% saline was injected intravenously after surgery, and the volume and rate changes were the same as those in Group R. We confirmed the return of neuromuscular function, which was defined as three consecutive train-of-four ratios ≥ 0.9, using a train-of-four monitor. Neuromuscular blockade was reversed with 0.004 mg kg− 1 glycopyrrolate and 0.02 mg kg− 1 neostigmine. Then, we verbally stimulated the patients every 30 s, and the patients were extubated once they regained consciousness and were able to obey verbal commands. The Sedation–Agitation Scale (SAS) was administered by independent anesthesiologists who were blinded to the anesthetic methods every 10 s. Finally, all patients were transferred to the post-anesthesia care unit (PACU) for close observation. A well-trained nurse blinded to the study groups evaluated pain intensity every 5 min using a numeric rating scale (NRS) (range: 0–10, with higher scores indicating worse pain). Nonsteroidal anti-inflammatory drugs were administered when the NRS score ≥ 5. Postoperative adverse events included hypotension, hypertension, bradycardia, tachycardia, postoperative nausea and vomiting (PONV), laryngospasm, cough, and hypoxemia. All adverse events were recorded from the end of surgery to discharge from the PACU. If such events occurred, intravenous injection of drugs such as ephedrine, urapidil, atropine, esmolol, and tropisetron was an option. Patients were discharged from the PACU when their Aldrete score was ≥ 9 [8]. The following evaluation time points were defined: T0, admission (basal); T1, at the end of the surgery; T2, after investigational drug infusion; T3, tracheal extubation; T4, 2 min after tracheal extubation; and T5, 5 min after tracheal extubation.
Outcome measurementsPrimary outcome
The primary outcome was the incidence of EA. Emergence was defined as the time interval from the end of surgery to 2 min after tracheal extubation. During emergence, EA was defined as an SAS score > 4 (1 = unarousable: no response to noxious stimuli; 2 = heavily sedated: aroused by physical stimuli but non-communicative; 3 = sedated: awakens to verbal commands or gentle shaking but drifts off again; 4 = calm: awakens easily, follows verbal commands; 5 = agitated: anxious or mildly agitated, calms down with verbal instructions; 6 = very agitated: requires physical restraint and frequent verbal reminders of limits; and 7 = dangerous agitation: pulling at tracheal tube, trying to remove catheters or striking staff [9].
Secondary outcomes
The secondary outcomes were as follows.
1.
The incidence of severe EA (defined as an SAS score of 7) and the maximal SAS score during emergence were also recorded.
2.
Recovery characteristics included extubation time, the length of the PACU stay, and the maximum NRS score in the PACU.
3.
Hemodynamic parameters (including MAP and HR) were recorded at six different time points: T0, T1, T2, T3, T4, and T5.
Postoperative adverse events included hypotension (MAP ≤ 70% of baseline and/or < 65 mmHg), hypertension (MAP ≥ 120% of baseline), bradycardia (HR ≤ 45 beats/min), tachycardia (HR of ≥ 120% of baseline) [10], PONV, laryngospasm, cough (0 = no coughing; 1 = single cough; 2 = persistent cough lasting < 5 s; 3 = persistent cough lasting ≥ 5 s), and hypoxemia (oxygen saturation < 90%).
4.
The incidence of postoperative delirium (POD) within 3 days after surgery was assessed using the Confusion Assessment Method [11].
Statistical analysis
The data processing and analyses were performed using SPSS 20.0 statistical software (IBM Corp., Armonk, NY, USA). All data are presented as mean ± SD number (%), or median (IQR) as appropriate. The normality of the data distribution was assessed with the Shapiro–Wilk test. Normally distributed data were compared between the groups using an independent-samples t-test, and non-normally distributed data were compared using the Mann–Whitney U test. The chi-square test or Fisher’s exact test was used for comparison of numerical data between the groups. The significance level for the analysis was set at α = 0.05.
A total of 40 patients completed the pre-experiment (20 patients in each group). The experimental protocol for the pre-experiment was consistent with that of the formal experiment. In the pre-experiment, the incidence of EA was 55% in Group C and 25% in Group R. Therefore, a sample size of 76 patients was needed to provide a power of 80% at a significance level of 0.05. Assuming a 10% attrition rate, we enrolled 86 patients in this study (43 patients in each group).


留言 (0)