The University of Iowa Institutional Review Board determined that this retrospective cohort study #202301239 does not meet the regulatory definition of human subjects research.
The time when the anesthesia provider extubated the patient was recorded using an extubation event button in the hospital's electronic health record (Epic Systems, Verona, WI) from Sunday, 9 October 2011, forwards. With the current study started in July 2023, there were 76 eight-week periods through Saturday, 3 June 2023. We studied every case at the University of Iowa (N = 182,374) that included general anesthesia, tracheal intubation in the operating room where the anesthetic was performed, tracheal extubation between 5 min before the end of surgery and the time of operating room exit, and absence of prone positioning. The University of Iowa is a large teaching hospital. The cases involved 574 distinct surgeons and 696 distinct anesthesia providers (Table 1) [13, 14].
Table 1 Characteristics of the 182,374 cases of the 574 distinct surgeons, 13,933 combinations of surgeon and eight-week period, and 23,958 combinations of surgeon, eight-week period, and binary of prolonged time to tracheal extubation or notExplanations of the independent variable and the three dependent variables
The binary independent variable’s threshold of 15-min is not arbitrary, and dichotomization does not lose economic information [15]. Anesthesiologists rated extubation times longer than 15 min as representing poor recovery from anesthesia [16]. That threshold was associated with immediate reintubation, respiratory treatments in the post-anesthesia care unit, and treatment with flumazenil and naloxone [17]. By 15 min after the end of surgery, non-anesthesia practitioners reliably were idle in the operating room waiting for extubation [18]. Briefer times to extubation generally were not associated with longer operating room times, because non-anesthesia practitioners have their own activities to be completed before the end of the case [18]. That is, a small delay in extubating during the interval while other personnel are performing activities that need to be completed before the patient can leave the operating room (i.e., parallel processing) do not result in an exit delay [18]. Unlike briefer extubation times, all (98/98) surgeons’ mean extubation times were exceeded by 15 min [2]. Finally, prolonged extubation times are largely preventable (see the first full section of the Discussion, below).
The first of the dependent variables was the interval in minutes from end of surgery to operating room exit. There was no censoring. Every patient included was intubated and extubated in the operating room and either had prolonged extubation or not. End of surgery was considered as the time recorded when the dressing was applied or, when not applicable or missing (e.g., rigid bronchoscopy, incomplete documentation), when the end of surgery was noted.
The total hours of cases, including the turnover times, in the operating room is the “workload,” as relevant to cost accounting. Turnover times are intervals from operating room exit to operating room entrance of the next case on the same day. For purposes of quantifying the room’s workload, cases starting between 6:30 AM and 7:30 PM on regular workdays were included. The second of the dependent variables was the proportion of prolonged extubations on regular workdays in operating rooms with workloads > 8 h. Turnover times longer than 120 min were counted as equaling 120 min because such extremely long turnovers are typically caused by a case cancellation or situation where the next case was not originally planned to be performed in the performed operating room (e.g., an add-on or case moved from another operating room). The third of the dependent variables was the turnover time among cases with the next case performed by the same surgeon on the same day and in the same operating room [1].
Statistical analyses by eight-week period and surgeon categories
Details of the statistical analyses are provided in Supplemental Table 1. These follow the order in the Results section. Patients’ dependent variables such as the daily workload are not statistically independent within or among surgeons because surgical cases are scheduled partly based on expectations of time in the operating room and the operating room’s workload [19,20,21,22,23]. That is, lack of independence occurs because the attributes of one patient (e.g., long duration surgical procedure) influences the attributes of the surgeons’ subsequent patients on the same day and subsequent days within the period of their “block” schedule. The University of Iowa used a four-week master surgical schedule, influencing surgeons’ operating days. Therefore, batches of eight-week periods were created, an integer multiple of the master schedule’s cycle [19,20,21,22,23]. The eight-week periods represent, statistically, a repeated measures analysis by surgeon. Statistical analyses were performed using Stata v18.0 (StataCorp, College Station, TX).
Our study of “surgeons” does not literally mean we evaluate surgeons, but rather the multiple behavioral decisions that are made in how patients get assigned to surgeons in clinics, how operating room cases are scheduled, and how trainees or experienced nurse anesthetists are assigned to surgeons [24, 25]. Similarly, intraoperative workflow at the end of surgery differs among surgeons because they perform different categories of procedures (e.g., head and neck versus gynecological laparoscopy) [2]. These factors matter for each of the three dependent variables.
Because the statistical analyses were performed by surgeon, all covariates in the model were surgeon characteristics. Surgeons were categorized broadly based on their patients’ ages and lengths of stay, provided the surgeon had at least 19 cases total, summed among all eight-week periods. Surgeons with most (> 50%) of their patients’ ages < 18 years were considered “pediatric surgeons.” Among the remaining surgeons, those with most of their patients admitted on the day of surgery and discharged before 11:59 PM of the day of surgery were considered surgeons with most of their practice being ambulatory surgery. Among the remaining surgeons, those with most of their patients undergoing a major therapeutic procedure [26] with an oncology diagnosis, based on their procedure’s International Classifications of Diseases, Ninth or Tenth Revision Clinical Modification diagnosis codes [27, 28], were considered surgeons with most of their practice being inpatient oncology surgery.
Statistical methods
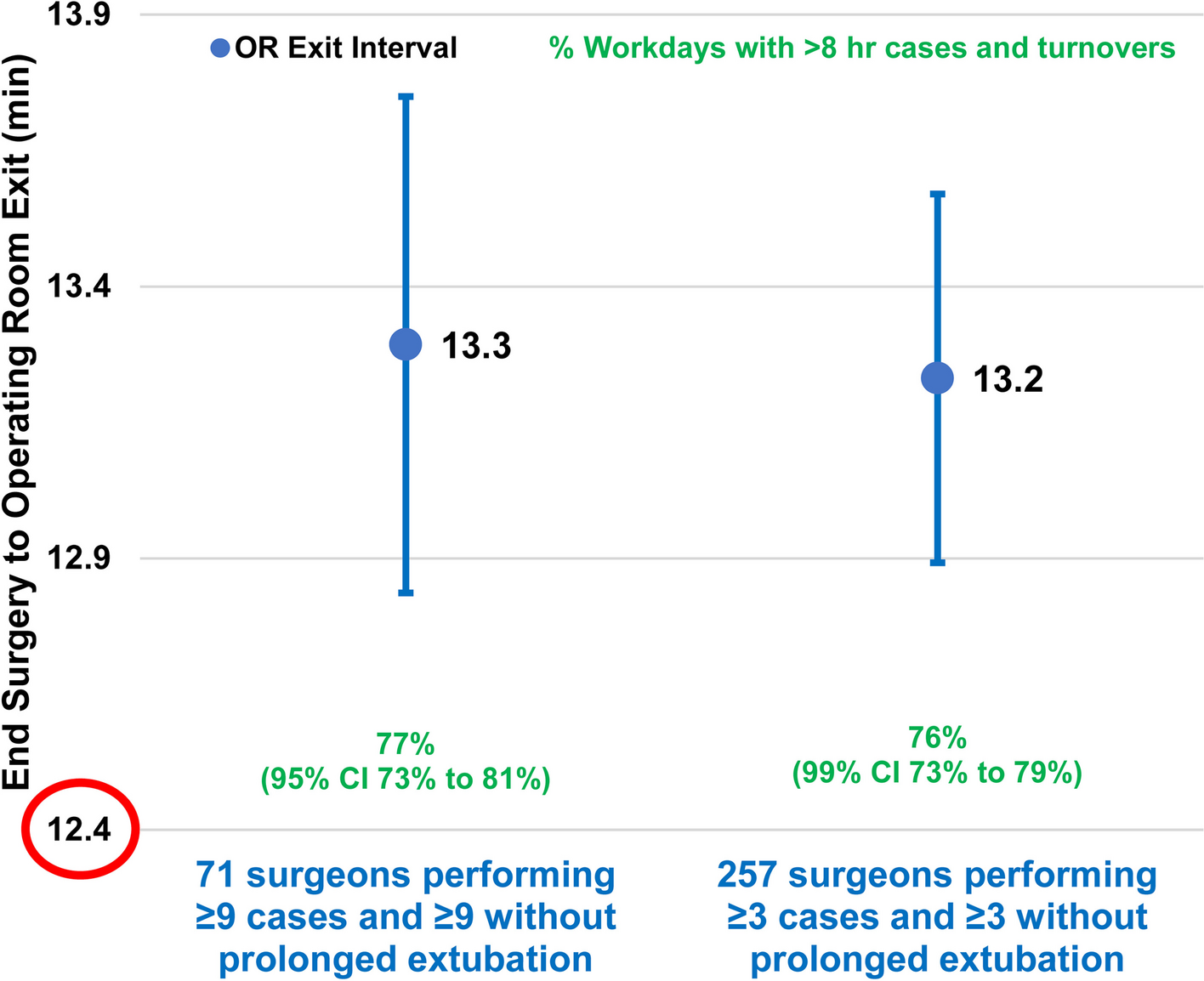
The first of the dependent variables was the interval in minutes from end of surgery to operating room exit. For each combination of the surgeon and eight-week period, the difference was calculated between (i) the mean operating room times after surgery ended among the cases with prolonged extubation and (ii) the mean among cases without prolonged extubation. Then, for each surgeon, the mean and the standard error of the mean were calculated over the eight-week periods during which they operated. (Standard errors, not standard deviations, are reported because weights in meta-analyses are calculated from the inverse of squares of the standard errors.) Thus, each surgeon had a point estimate of the mean difference and a corresponding standard error. The mean differences were then pooled among surgeons to obtain the final estimate, using a random intercept model. The variance of the model was estimated using the DerSimonian-Laird method [29, 30]. Knapp-Hartung adjustment was made for the sample size of surgeons [31, 32]. This random-effects analysis was performed primarily among the combinations of surgeons and eight-week periods with at least nine cases with prolonged extubation and at least nine that were not. The criterion for statistical significance was that the two-sided P < 0.05. Similarly, 95% two-sided confidence intervals were calculated. Sensitivity analyses were calculated using three subgroups of surgeons (pediatric surgeons, surgeons with primarily ambulatory surgery cases, and cancer surgeons) and using two different numbers of observations per eight-week period (≥ 3 and ≥ 19). For the sensitivity analyses, to adjust for the five comparisons, P < 0.01 was treated as statistically significant, and 99% confidence intervals were used.
The second of the dependent variables was the proportion of prolonged extubations in rooms with > 8 h of cases and turnover times. Because the observed percentage was 57% in the earlier study [3], a value significantly greater than 50% was expected but vastly less than 90%. Arcsine transformation was made of the observed proportion for each combination of the surgeon and eight-week period. [13, 19, 23, 33,34,35],Footnote 1 The mean and standard error of the mean were calculated over the eight-week periods for each surgeon. Then, random intercept meta-analysis was used to estimate the overall mean and confidence interval among surgeons. The inverse transform was then reported.
The third of the dependent variables was turnover times. Analyses were planned to be like the first of the three dependent variables (i.e., interval from end of surgery to room exit). However, we knew that the sample size would be much smaller because an earlier study at the hospital [36], and studies of all hospitals in the states of Iowa and Florida [37,38,39,40], showed that most surgeons’ cases are not followed by another case of the same surgeon that day.
We had a priori criteria for the appropriateness of the sample size for the first and second of the three dependent variables. In the earlier papers from 2013, a mean difference in the time from the end of surgery to room exit exceeding 5 min was considered economically important [2]. That is not to say that briefer times would be unimportant, but rather that hospitals reliably would try to save an average of 5 min with teams working late. Therefore, we would consider our sample size sufficient if the resulting confidence interval for the mean difference excluded plus and minus 5 min (e.g., the lower limit exceeded 5 min) [2]. We expected that criterion to be satisfied because, in the 2013 paper, the standard error of the mean was 0.6 min although there were many fewer cases (72,051 versus the current study’s 182,374) and surgeons (98 versus the current study’s 574) [2]. The minimum of 5 min matters economically when the workload is large, ≥ 8 h. At most (> 50%) surgical facilities nationwide, most operating rooms have ≤ 8 h of cases and turnover times [7,8,9,10]. We tested the fractions based on 50%, that most of the prolonged extubations occurred in operating rooms with > 8 h of cases and turnovers [3]. We expected the sample size sufficient to test “most” because our previous studies had much smaller sample sizes and yet reliably detected significant difference [3].
Statistical analyses were repeated using mixed effects models to evaluate if estimates were similar. The random effect was the surgeon. Prolonged extubation was treated as a fixed effect. The eight-week periods were entered as a centered, continuous variable (i.e., the overall mean by case within each period was subtracted from each value during that period). Robust variance estimation was used. These results were secondary for two reasons. First, the mixed effects model assumes homogeneity of the effect of prolonged extubation among surgeons, known, a priori, to be false. Second, the mixed effects model treats the dependent variables of the cases of the same surgeon to be statistically independent, although that is not true for cases within periods because of staff scheduling and assignment [13]. For example, for the second dependent variable of the duration of the workday, the sample size of the mixed effect logistic regression model was the number of cases. Thus, three cases on the same day in the same operating room with > 8 h of cases and turnovers would contribute N = 3 although the cases encompass one scheduled workday.


留言 (0)