
記住我

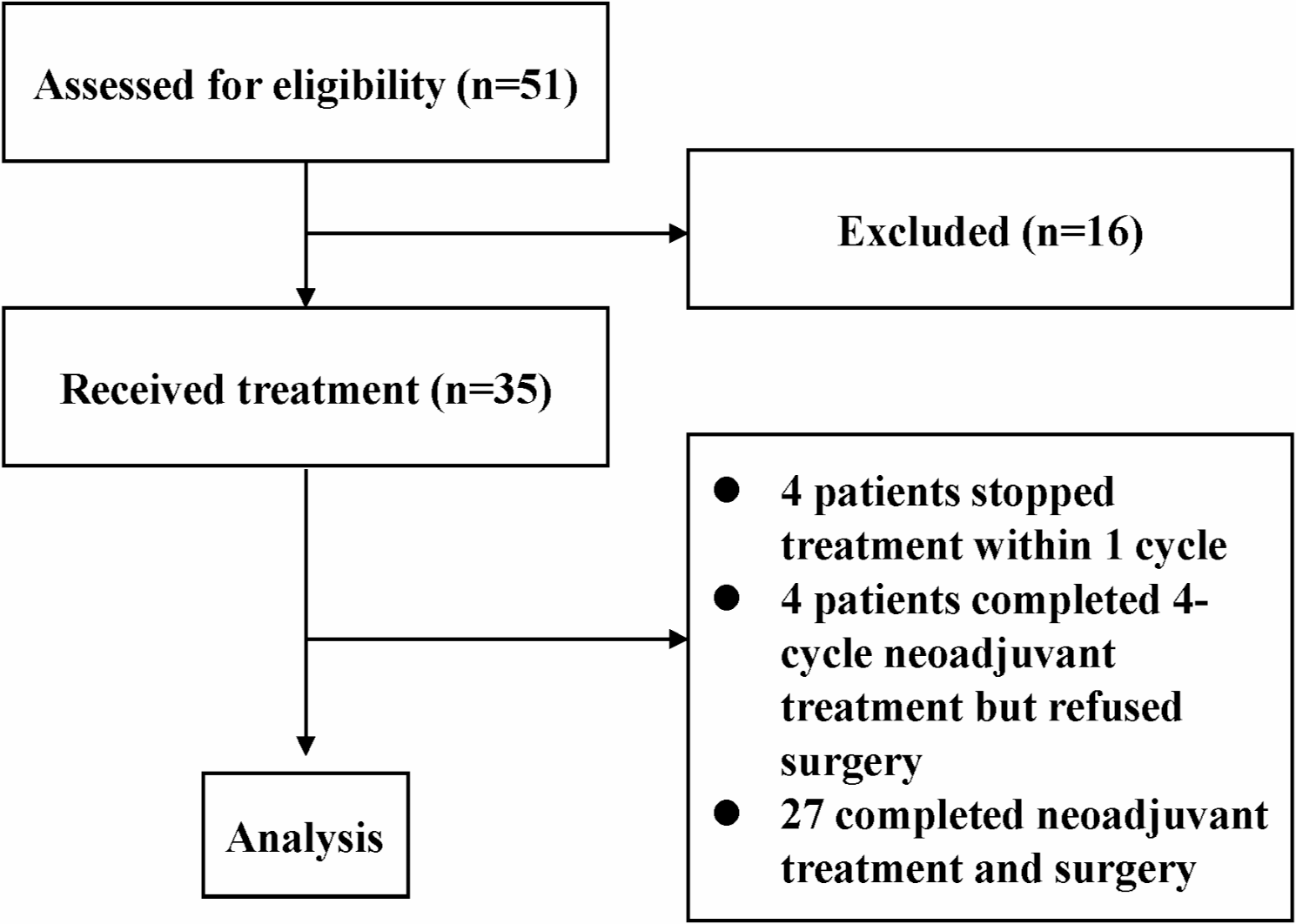



Cohort: A retrospective cohort of women diagnosed by needle or incisional biopsy with loco-regional invasive, non-inflammatory breast cancer between 2010 and 2017 in the SEER-Medicare database who received surgery as their first treatment was selected. The SEER-Medicare linked database combines Medicare Parts A and B claims with clinical and outcome data from SEER cancer registries [17]. Medicare is a federal health insurance program available for individuals 65 and older and some individuals younger than 65 with specific disabilities or conditions [18]. All data were de-identified and met the criteria for exempt review by the University of Oklahoma Health Sciences Center Institutional Review Board (IRB7446). Patients younger than 66 were excluded due to the bias presented by the enrollment criteria for those under 65 and lack of claims history for patients who qualified for enrollment based on age in the same year as their diagnosis. Patients who had HMO coverage or did not have continuous Part A and B coverage for at least one year prior through one year after diagnosis were excluded due to the inability to accurately ascertain existing comorbidities at the time of diagnosis or full claims for the primary course of treatment. Patients who received surgery within 7 days of diagnostic biopsy were excluded since the time required for pathologic molecular diagnosis commonly takes up to one week [19]. Additionally, patients that did not receive surgery until over ≥ 120 days after diagnosis, had a time of death less than one year after surgery, SEER reported follow-up shorter than TTS, non-definitive initial surgery (i.e., re-excisions), prior cancer diagnosis, non-locoregional disease (i.e., in situ, regional direct extension, or distant metastatic spread), or missing information were excluded (Fig. 1).
Fig. 1
Exposure: The primary exposure, time-to-surgery (TTS), was defined as the days from the date of diagnostic biopsy to the date of surgery.
Outcome: Breast cancer-specific mortality (BCSM) in the presence of competing events (i.e., death from other causes) was assessed, and survival times were calculated from the date of surgery to death or last contact (censored).
Definitions: Loco-regional breast cancer (see Appendix) is defined by the SEER summary as a localized disease confined to breast tissue and fat, including the nipple and/or areola; regional lymph node involvement is defined as axillary (levels I–III), infraclavicular (subclavicular), internal mammary, intramammary, or other regional lymph nodes not otherwise specified. The cohort was stratified by hormone receptor (i.e., estrogen and/or progesterone receptor; [HR]) and HER2 status into 3 groups: HR + /HER2 −, HR −/HER2 −, and HR + or HR −/HER2 + [HER2 +]. Age at the time of diagnosis was categorized in 5-year intervals (i.e. < 70, 70–74, 75–79, 80–84, and ≥ 85 years old). Race/ethnicity was categorized as non-Hispanic Black (Black), other (Asian, Hispanic, Pacific Islander, American Indian/Eskimo/Aleutian, and other non-specified race or ethnicity), or non-Hispanic White (White). The Charlson Comorbidity Index was calculated for each patient using the SEER-Medicare developed Comorbidity SAS Macro [20] (2021 version) to search for relevant claims in the year prior to diagnosis, and classified as 0, 1, or ≥ 2. Education (% of residents without high school degree) and residential median income were based on census tract level information from the 2010 U.S. Census and the patient’s census tract of residence at the time of diagnosis. Histology was categorized as ductal, lobular, or other by ICD-O-3 codes (Appendix 1). The HCPCS, ICD-9, and ICD-10 codes used to classify diagnosis, surgery, and adjuvant therapies in Medicare claims are listed in Appendix 2. The surgery type was classified as breast-conserving, mastectomy, or mastectomy with immediate reconstruction.
Statistical methods: Time to death as a function of TTS was analyzed separately by subtype using Fine-Gray competing risk models for BCSM. All models were adjusted using inverse propensity score weights (IPW) to account for potential imbalances in covariates associated with TTS [21,22,23]. Covariate balancing propensity scores were computed using the R package “CBPS” with socio-demographic (age at diagnosis, race/ethnicity, census tract median income, and census tract % without a high school degree) and clinical factors (Charlson Comorbidity Index, year of diagnosis, SEER combined summary stage, histology grade, type of surgery, histology) as predictors and log-transformed TTS as the response variable [23]. Pre-/post-weighting balance was assessed for each model using Love plots. Final survival models were adjusted by normalized IPW, with extreme weights beyond the 95th percentile winsorized, along with receipt of adjuvant radiation or systemic therapy, comorbidity score, and, in HER2 + patients, hormone receptor status. B-splines were used to flexibly model the subdistribution hazard of mortality as nonparametric functions of TTS. Subdistribution hazard ratio (sHR) estimates were calculated using TTS = 30 days as the reference point since it is commonly used as the upper limit of the reference in categorical TTS studies [13, 15, 24]. Simultaneous 95% confidence intervals (CI) at each TTS point were computed using the Scheffe method. The association between TTS and sHR was considered significant when the simultaneous 95% CI did not include a subdistribution hazard ratio of 1. To provide estimates of the BCSM incidence at TTS of 30, 60, 90, and 120 days, the adjusted cumulative incidence function was derived from the Fine-Gray model conditioned on the subgroup of patients with the most common characteristics. The Wilcoxon rank sum test was used to compare the median TTS differences between race groups. The Jonckheere trend test [25] was used to test the increasing trend in median TTS by diagnosis year. All statistical analyses were conducted using SAS (version 9.4; Cary, NC) and R software (version 4.0.4), and graphs were generated using JMP Pro 15.2.0 (SAS; Cary, NC).
留言 (0)