The acquisition and use of this dataset, which exclusively comprises routinely collected data, was approved by the local ethics committee (REC 23/YH/0085). The dataset includes high-resolution monitoring data and clinical descriptors from consecutive TBI patients admitted to the Neurocritical Care Unit at Addenbrooke’s Hospital, Cambridge University Hospital NHS Foundation Trust, University of Cambridge. Data acquisition occurs continuously while the patient remains in the NCCU and respective monitoring is deemed necessary. If care is redirected—for example, to palliative measures—monitoring is discontinued. For all other cases, monitoring continues for the entirety of the patient's stay in the unit. This approach ensures comprehensive data collection during active treatment. All data were obtained as part of routine care, encompassing invasive neuromonitoring and regular physiological monitoring. No additional study-specific data were collected, and therefore, the requirement for informed consent was waived.
Study population
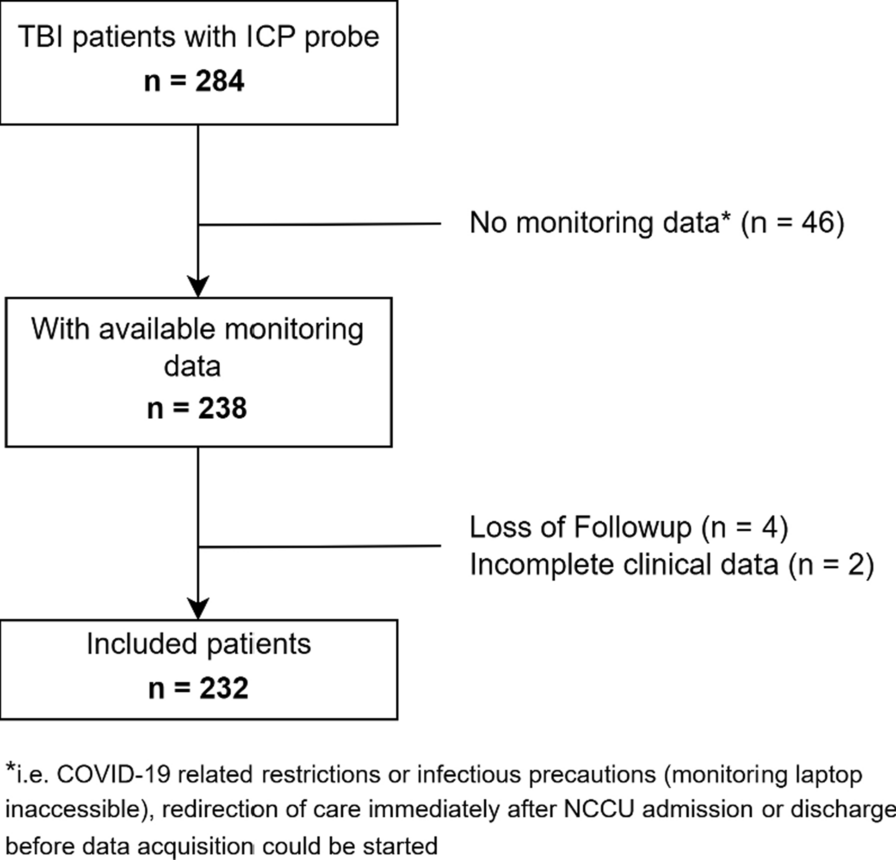
Patients admitted between 03.2021 and 12.2023 were evaluated for inclusion. Inclusion criteria were: 1. Acute TBI with invasive ICP monitoring; 2. Available 6-month outcome (Glasgow Outcome Scale – GOS). The exclusion criteria were: 1. No monitoring data; 2. loss of follow up with missing 6-month outcome; 3. Incomplete clinical descriptors. Patients were treated based on previously described protocols [13, 14] and in accordance with the guidelines by the Brain Trauma Foundation [15].
Data acquisition
High resolution physiological data (250 Hz) was collected in real time at the bedside using the ICM + software running on a laptop at the bedside (ICM + software ®, Cambridge Enterprises, University of Cambridge, UK). ICP was measured using intraparenchymal wires (Codman ICP MicroSensor, Codman & Shurtleff, Raynham, Massachusetts). ABP was measured using arterial lines (Baxter Healthcare, Deerfield, Illinois) inserted to the radial or femoral artery and zeroed at the level of the foramen of Monroe. The following clinical data was extracted from the database: sex, age, Glasgow Coma Scale (GCS), pupillary reactivity (both reactive vs. one reactive vs. none reactive), presence of intracranial bleeding (extradural hematoma—EDH, intracerebral hematoma—ICH, subdural hematoma—SDH, contusion, traumatic subarachnoid hemorrhage—SAH), presence of extracerebral injuries (divided into injuries to thorax, abdomen, extremities, pelvic, skull, or spine), presence of isolated TBI (no extracranial injuries), decompressive craniectomy (DC), and GOS. GOS was assessed at 6 months after ictus during outpatient consultations or via telephone interviews by trained staff. Outcome was evaluated assessing the ordinal scale (good recovery vs. moderate disability vs. severe disability vs. dead/vegetative) or as dichotomized outcome (GOS 1–4 vs. 5–8) or dead/vegetative vs. other outcome categories (GOS 1/2 vs. 3–8).
Data preprocessing
The high-resolution (i.e. waveform) monitoring data was preprocessed using ICM+. Raw ABP and ICP signals were curated to remove the following artifacts: 1. Sections with arterial line failure (continuous reduction of the arterial blood pressure amplitude followed by flushing) were removed manually; 2. Values of ABP below 0 or above 300 mmHg and sections with a pulse amplitude below 15 mmHg were removed automatically; 3. Values of ICP below -30 or above 200 mmHg, with low amplitude (< 0.04 mmHg) or with a 95% Spectral edge frequency above 10 Hz (high-frequency noise) were removed automatically. Based on the curated data, heart rate (HR – calculated by extracting the fundamental frequency of ABP within the limits of 40 to 180 beats per minute) and ICP amplitude (AMP – fundamental amplitude of ICP within the limits of 40 to 180 beats per minute) were estimated. The resulting artifact free data was then processed to acquire 10 s averages of ABP, ICP, AMP, CPP (difference between ABP and ICP), and HR. For ABP and ICP this coarse-graining removes the cardiac and respiratory components of the signal.
Multiscale entropy analysis
MSE was calculated as previously described [4, 16]. Sample entropy [17] was calculated for a total of 20 steps (with 1 being the raw data and each consecutive step describing the number of consecutive samples to be averaged leading to coarse graining of the data) with a sequence length of m = 2 and a tolerance of 0.15. Sample entropy estimates whether corresponding sequences of length m remain the same when extending the sequence by one sample (i.e. m + 1). Its value is the negative natural logarithm of the ratio between the number of m + 1 length and corresponding m patterns. The resulting area under the curve (AUC) of the plotted sample entropies at all steps was termed MSE. Increasing MSE represents increasing entropy and thus complexity of the signal. To allow for the analysis of time-trends, MSE was calculated every 5 min for consecutive overlapping 6 h data segments with a minimum of 1000 valid samples. MSE was calculated for each of the biosignals resulting in the metrics MSE abp, MSE cpp, MSE hr, MSE icp, and MSE amp. In addition to the overall levels of MSE, percentage monitoring time (ptime) or dose (area below the curve) below specified MSE cutoffs [9, 12, 15] were calculated relative to the amount of available artefact free monitoring data. The thresholds were defined based on previous reports of MSE and based on an initial exploration of the distributions.
Statistical analysis
Statistical analysis and figure preparation was performed in R Studio (R version 4.3.2—https://www.r-project.org/—packages used: gtsummary, rstatix, MatchIt, cobalt, lme4, MASS, Hmisc, ggplot2).
Descriptive variables are reported as counts (percentages) or median (interquartile range – IQR). Different statistical methods were explored to assess the association between MSE dose or ptime and outcome. Univariable, multivariable, and ordinal analyses were performed. A significance level of p < 0.05 was set, without adjustment for multiple testing due to the exploratory nature of the study and the different tests used for exploration.
Univariable tests: First, the different MSE variables were compared to outcome using Kruskal–Wallis tests assessing group level differences and then using Wilcoxon rank sum tests comparing between subgroup differences. The diagnostic performance of the metrics was assessed by plotting their receiver operating curves and extracting AUC, and the derived measures sensitivity, specificity, and accuracy (based on the Youden index).
Multivariable tests: Two multivariable approaches were used to assess the relevance of the MSE metrics when corrected for known predictors of outcome in TBI. First, we applied propensity score matching to account for covariates [18]. The propensity scores were estimated using logistic regression comparing favorable vs. unfavorable outcome. The following parameters were included to estimate the propensity scores: age, sex, motor GCS, pupillary reactivity, type of hemorrhage – EDH/ICH/SDH/contusion/SAH, isolated TBI vs. polytrauma, extracranial injury (to the abdomen, extremities, pelvis, skull, spine, or thorax seperately), and DC. Propensity score matching was performed using the nearest-neighbor method with a caliper of 0.2 and 1:1 matching to ensure that matches were within a reasonable distance in terms of their propensity scores. Quality of the matching procedure was verified visually (density and point distribution plots) and quantitatively (evaluation of absolute mean difference before and after matching and basic statistical analysis). The different MSE metrics were then fed into multivariable logistic regression models including other multimodal monitoring metrics (i.e. average ICP, CPP, PRx). Second, a sliding dichotomy approach [18] was applied. The sliding dichotomy approach creates a relative outcome scale for each patient. The definition of favorable and unfavorable outcome is adjusted depending on the propensity score (calculated as described above) for each patient. For patients with excellent prognosis at admission, only GOS 5 is considered favorable, while for patients with poor prognosis at admission, survival would already be regarded as a favorable outcome. Based on the propensity scores, the patients were divided into three groups of roughly equal size with low, intermediate, and high likelihood of unfavorable outcome. The definition of favorable and unfavorable outcome was then adjusted for each patient. In patients with low likelihood only GOS of 5 was considered favorable, while for the patients with intermediate likelihood GOS of 4–5 and for the patients with high likelihood GOS of 3–5 was considered favorable. The patients were then assessed using logistic regression based on this adjusted outcome definition. Additional secondary multivariable analyses were performed to further explore the value of the MSE metrics: 1. A second multivariable propensity score matching based approach was explored including ICP, CPP and PRx doses instead of averages to mimic the dynamic assessment of MSE explored in this analysis. For this purpose, patients were matched as described above and then compared using multivariable regression models including ICP, CPP and PRx doses (i.e. ICP dose above 20 mmHg, CPP dose below 60 mmHg, PRx dose above 0.3) and either MSE metric. 2. A backwards stepwise elimination regression was performed. In light of the moderate sample size with various known clinical and monitoring metrics associated with outcome, the backward stepwise elimination process was chosen since it allows for automated simplification of models (with many initially added variables), retaining only the key predictors of outcome. The initial model was built including the various clinical metrics (age, sex, motor GCS, pupillary reactivity, type of hemorrhage – EDH/ICH/SDH/contusion/SAH, isolated TBI vs. polytrauma, extracranial injury (to the abdomen, extremities, pelvis, skull, spine, or thorax separately), DC), the multimodality monitoring metrics (ICP, CPP, PRx) and either MSE metric. 3. To provide a quantification of improvement of the models when including the MSE metrics, we also explored the continuous net reclassification index [19]. The continuous net reclassification index represents the proportions of individuals correctly reclassified (true positive or true negative), minus the proportion misclassified when comparing new to old models. Considering the number of patients available the initial model included ICP dose above 20 mmHg, CPP dose below 60 mmHg, and PRx. This model was then compared to a model including the described metrics as well as one of the MSE metrics.
Time trends: Time trends were first explored visually exploring consecutive 6-h non-overlapping averages of the different MSE dose and ptime metrics. To adjust for possible non-linear changes, generalized additive models (GAM) were used to investigate the relationship between MSE metrics, day, and outcome. Formal statistical analysis was then performed using mixed effects model assessing the MSE metric trajectories depending on the fixed effects day and outcome including the patient as a random effect. Additionally, to explore whether differences were apparent early on, the entropy metrics were compared using the Kruskal–Wallis rank sum tests considering only the data acquired within the first 24 h after injury.
Correlations: To explore the possible physiological origin of the changes in MSE metrics, correlation coefficients between MSE metrics and different variables were estimated. For these estimations, we assessed the MSE as well as the physiology metrics considering the complete period available. Pearson correlation was used for continuous variables and Spearman correlation for ordinal metrics. The MSE metrics were correlated to the available clinical metrics described in the sections above. Additionally, the metrics were correlated to absolute mean HR, ABP, CPP, and ICP. Additionally, the following metrics were calculated and assessed: CPP dose and ptime below 60 mmHg, ICP dose and ptime above 20 mmHg. Cerebrovascular autoregulation was estimated using the proxy measure PRx [20] (absolute value as well as dose and ptime above 0.3) and its derivatives describing the optimal CPP (CPPopt) [21], and the lower limit of autoregulation (LLA) [22]. Lastly, individual episodes of CPP, ICP, or PRx insults were extracted and analyzed. Insults were defined as follows: a CPP insult was characterized by a decrease in CPP drop from above 60 mmHg for at least 15 min; an ICP insult was defined as an increase in ICP to above 20 mmHg for at least 15 min; and a PRx insult was identified by an increase in PRx to above 0.3 for at least 30 min [23] to allow for a sufficient change in biosignal state. MSE metrics, comparing the hour before and the hour after onset of each insult, were analyzed using paired t-tests and linear mixed-effects models. These models were adjusted for patient-specific random effects and included MSE and insult intensity (e.g., the change in CPP before vs. during the insult) as fixed effects. To further characterize the temporal relationship between MSE and the insults, cross-correlation analyses were performed (allowing a bidirectional lag of up to 30 min) to quantify the degree of similarity between the two timeseries as a function of a time lag, enabling the determination whether changes in MSE precede, coincide with, or follow the occurrence of changes in cerebral biosignals.


留言 (0)