
記住我

Data from 288 prospectively enrolled sepsis patients were analyzed. The median age was 63 years (IQR 56–72.9) and 53% of participants were male. Among enrolled patients, 51% were Black and 46% were White. The most common comorbidities were diabetes mellitus, chronic obstructive pulmonary disease, and end-stage renal disease. Median total cholesterol, HDL-C, and LDL-C levels for the whole cohort were 91.6 (IQR 74–122), 26 (IQR 15–38), and 40.4 (IQR 26.0–61.0) mg/dL, respectively. The median SOFA score for the overall cohort was 7 (IQR 4–10), and nearly half of all patients were mechanically ventilated, while over one-third required vasopressors. Twenty-eight-day mortality was 22%. Demographics, cholesterol levels, and clinical features are presented in Table 1. Sources of infection are presented in Supplemental Table 1.
Table 1 Clinical features and cholesterol levelsHYPO patients were clinically discernible from NORMO patients in several ways. A Seaborn clustermap provides a visual representation of the 15 defining features of HYPO and NORMO subphenotypes (Supplemental Fig. 1). The 15 features included triage temperature, triage systolic blood pressure, total cholesterol, LDL-C, HDL-C, paraoxonase-1 (PON1) activity, apolipoprotein (ApoA-I) levels, coagulation SOFA, intercellular adhesion molecule-1 (ICAM-1) level, hepatic SOFA, renal SOFA, total SOFA, cardio SOFA, neuro SOFA, and respiratory SOFA. HYPO patients exhibited lower total cholesterol (78, IQR 64–97.3 vs. 107, IQR 87–133.8, p < 0.001), HDL-C (18, IQR 10–30.9 vs. 32, IQR 20–42.5, p < 0.001), and LDL-C (29, IQR 19.5–42 vs. 48.5, IQR 34.1–71, p < 0.001) levels (mg/dL, Table 1) compared to NORMO. HYPO patients also had higher median SOFA scores (9, IQR 7–11 vs 5, IQR 4–7.5, p < 0.001), increased vasopressor use (67% vs 34%, p < 0.001), longer ICU lengths of stay (4 vs 3 days, p = 0.001), and higher 28-day mortality (30% vs 16%, p = 0.004) (Table 1) compared to NORMO. There was no significant differences in statin use vs. non-use in HYPO vs. NORMO patients, and there were no associated differences in SOFA score or mortality (Supplemental Table 2).
Fig. 1
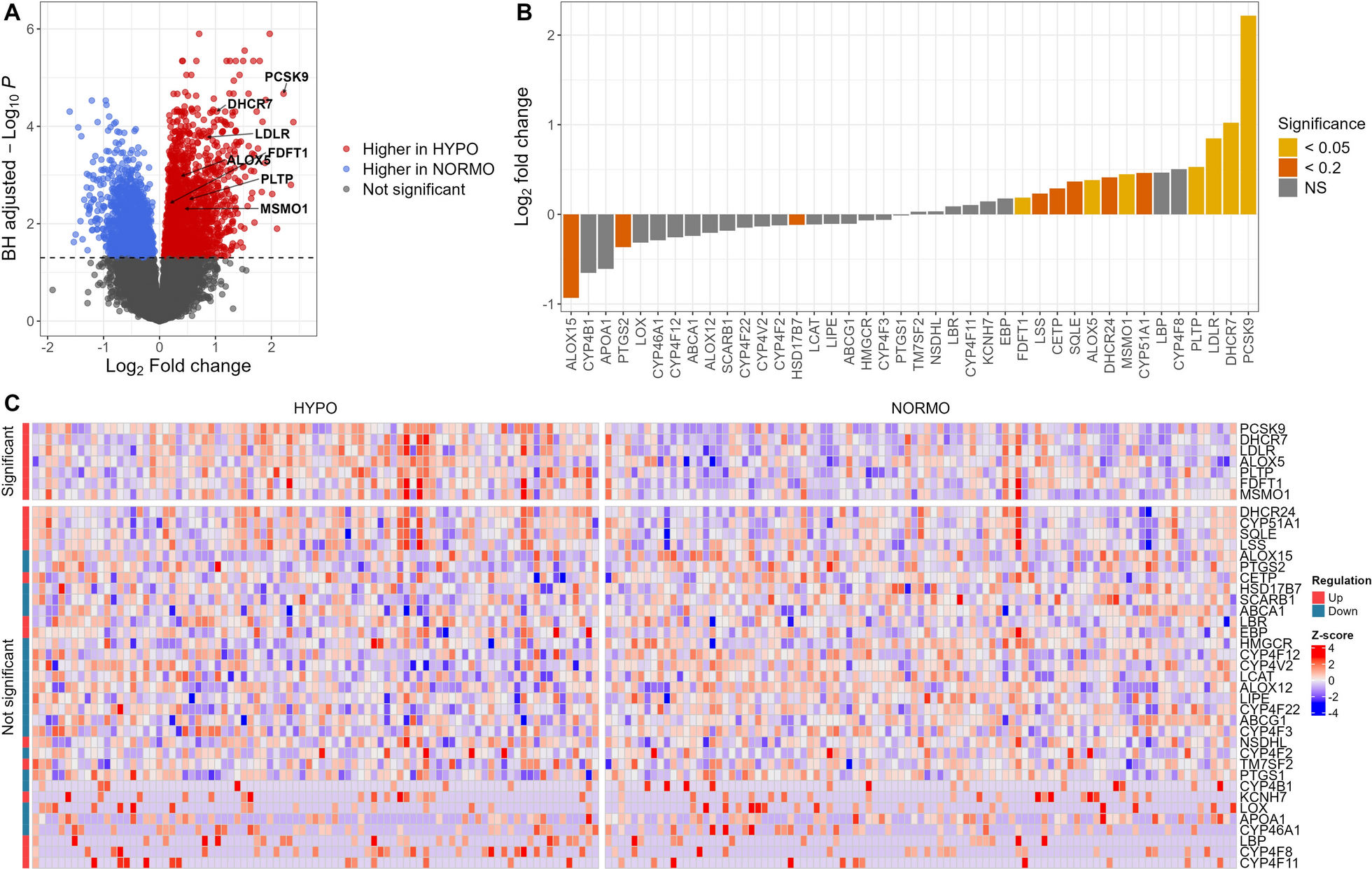
RNA-seq analysis comparing HYPO vs. NORMO. A Volcano plot displaying results from the differential expression analysis of 26,878 genes between HYPO and NORMO. Each dot represents a gene, with colors indicating significance, using a Benjamini-Hochberg-adjusted P value cutoff of less than 0.05 (dashed line). The x-axis denotes the log2 fold change for HYPO vs. NORMO, and the y-axis shows the Benjamini-Hochberg-adjusted -log10 P value. B Bar plot showing the log2 fold change of 40 lipid genes for HYPO vs. NORMO. Seven non-expressed lipid genes have been excluded from the analysis. Colors represent the significance of these genes, determined by the Benjamini-Hochberg-adjusted P value, adjusted for 26,878 comparisons. C Heatmap showing the expression of 40 lipid genes. Seven non-expressed lipid genes have been excluded from the analysis. The color scale corresponds to z-scored, log2-transformed gene expression values for each sample. Significance was determined by the Benjamini-Hochberg-adjusted P value, with a cutoff of 0.05, adjusted for 26,878 comparisons
Table 2 Differentially expressed lipid metabolism genesRNAseq was conducted on samples from 184 patients. Of these, 87 (47%) were classified as HYPO and 97 (53%) were NORMO. Seven lipid metabolism genes were upregulated in HYPO (Table 2) compared to NORMO patients. These genes were Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9), 7-Dehydrocholesterol Reductase (DHCR7), Low-Density Lipoprotein Receptor (LDLR), Arachidonate 5-Lipoxygenase (ALOX5), Plasma Phospholipid Transfer Protein (PLTP), Farnesyl-Diphosphate Farnesyltransferase 1 (FDFT1), and Methylsterol Monooxygenase 1 (MSMO1). The volcano plot (Fig. 1A) illustrates upregulated genes, with lipid genes annotated, in HYPO vs. NORMO patients. Figure 1B demonstrates the relative up vs. downregulation of each gene contributing to the HYPO vs. NORMO subphenotypes. Figure 1C displays a Seaborn clustermap of gene expression by subphenotype. Of the 47 a priori lipid-related genes of interest (Supplemental Table 3), 37 were cataloged in the KEGG database. The primary pathways associated with these significant genes include steroid biosynthesis, cholesterol metabolism, and arachidonic acid metabolism as detailed in the Supplemental Data File. Three additional KEGG pathways—ovarian steroidogenesis, serotonergic synapse, and efferocytosis—were also enriched in our analysis when using significance criterion for significant genes to an adjusted p = 0.2. Supplemental Fig. 2 displays boxplots of the upregulated genes in HYPO vs. NORMO patients as well as the mean contribution of each gene to the HYPO subphenotype via the Gini coefficient (GC).
Fig. 2
Lipidomics analysis comparing HYPO vs. NORMO. A Heatmap showing the abundance of 13 lipid classes analyzed via shotgun lipidomics. The color scale corresponds to z-scored concentration values for each sample. Significance was determined by the Benjamini-Hochberg-adjusted P value, with a cutoff of 0.05, adjusted for 13 lipid class comparisons. B Ridgeline plot comparing lipid species between HYPO and NORMO. Each dot represents an individual lipid species within its corresponding lipid class (y-axis). The color of the dot indicates whether the lipid is significantly altered, with a cutoff of 0.05 for the Benjamini-Hochberg-adjusted P value, adjusted for all 355 lipid species comparisons. The x-axis represents the log2 fold change for HYPO vs. NORMO. Four lipid classes (PA, LacCER, PG, and PS) are hidden due to having fewer than 3 individual lipid species within the class. C Volcano plot displaying the differential abundance of 355 lipids between HYPO and NORMO. Each dot represents a lipid species, with colors indicating significance using a Benjamini-Hochberg-adjusted P value cutoff of less than 0.05. The x-axis denotes the log2 fold change for HYPO vs. NORMO, and the y-axis shows the Benjamini-Hochberg-adjusted -log10 P value
Shotgun lipidomics analysis was performed on 271 patients, with 116 (43%) classified as HYPO and 155 (57%) classified as NORMO. HYPO patients showed significantly lower levels of specific classes of lipids including cholesterol esters (CE, adjusted p < 0.001), sphingomyelins (SM, adjusted p < 0.001), and lysophosphatidylcholines (LPC, adjusted p < 0.001) (Supplemental Table 4). Individual lipids that were significantly different between classes are displayed in Supplemental Table 5, most of which had lower levels in HYPO vs. NORMO patients. Figure 2A shows the Seaborn clustermap of lipid classes by HYPO vs. NORMO subphenotype. Figure 2B shows the differences in lipid classes between HYPO and NORMO subphenotypes, while Fig. 2C demonstrates the log2 fold change in individual lipid moieties between HYPO vs. NORMO patients. Our signaling lipid panel was conducted on 257 patients, with 111 (43%) classified as HYPO and 146 (57%) classified as NORMO. However, the results were not statistically significant between the two cohorts for any signaling lipids (Supplemental Table 6).
To better understand the association between upregulated genes by subphenotype, and specific lipids in the shotgun lipidomics experiment, we visually presented these data using a correlation matrix (Fig. 3). Here we can see that the influence of gene expression differences between HYPO and NORMO subphenotypes on individual lipid levels becomes apparent. Specifically, DHCR7 and LDLR upregulation in the HYPO cohort was strongly correlated with reduced levels of CE 14:0, 16:0, 16:1, CE 18:0, CE 18:1, CE 18:2, and CE 20:3, compared to the NORMO cohort. Upregulation of PCSK9, MSMO1, DHCR7, PLTP, and LDLR in HYPO patients was also more strongly correlated with upregulation of LPC’s 18:0, 18:1, and 18:2 compared to NORMO patients overall. DHCR7 upregulation in HYPO was also most strongly correlated with low SM levels, specifically d18:1/22:1 and d18:1/24:0. Interestingly, PCSK9 expression in NORMO patients was more strongly associated with low SM levels than in HYPO patients and was also significantly associated with low LPCs.
Fig. 3
Correlation analysis between individual lipids and HYPO vs. NORMO subphenotypes by expression of the 7 significant genes. The correlation matrix displays significant correlations between genes in overall analysis (all patients, N = 168), HYPO patients only (N = 79), and NORMO patients only (N = 89), for patients with RNAseq data. Significant correlations are indicated as follows: ***p < 0.001, **p < 0.01, *p < 0.05). Differences in the correlations between specific upregulated genes and individual cholesterol esters (CE), lysophosphatidylcholines (LPC), phosphatidylcholines (PC), and sphingomyelins (SM) are observable between HYPO and NORMO patients, with the most significant differences correlated with upregulation of PCSK9, MSMO1, DHCR7, PLTP, and LDLR in HYPO patients
We compared the long-term survival of HYPO vs. NORMO patients. Using the log-rank test with 95% confidence intervals and comparing survival of patients out to 1 year, 6-month survival was 63.7% (95% CI 54.5–74.5) for HYPO patients, and 78.6% (95% CI 71–87) for NORMO patients (p = 0.0085). At one year, survival was 56.2% (95% CI 46.1–68.6) for HYPO patients and 73% (95% CI 64.4–82.7) for NORMO patients (p = 0.0067, Supplemental Fig. 3).
External dataset comparisonsDifferential expression analysis was conducted on two external datasets [32, 33]. The study by Scicluna et al. included sepsis patients who were admitted to two ICUs in the Netherlands, and described four phenotypes based on gene expression patterns, designated MARS 1, 2, 3, and 4. Patients with MARS 1 or 2 phenotypes had the highest burden of organ failure, shock, and the highest mortality compared to patients with MARS 3 or 4 phenotypes. We performed differential expression analysis on 479 MARS sepsis patients focused on our 47 a priori lipid metabolism genes. Comparing 28-day non-survivors to survivors, non-survivors had upregulation of two lipid metabolism genes TM7SF2 and APOA1 at the adjusted p < 0.05 level, and five genes FDFT1, LDLR, MSMO1, EBP, and LOX at adjusted p < 0.2. Three of these genes, FDFT1, LDLR, and MSMO1, were the same as those identified in the HYPO subphenotype. When comparing the more severe MARS 1 and 2 patients to MARS 3 and 4 patients, MARS 1 and 2 patients had upregulation of six of the seven genes as our HYPO subphenotype including ALOX5, FDFT1, LDLR, MSMO1, DHCR7, and PCSK9 at adjusted p < 0.05. We subsequently applied the random forest models to predict HYPO and NORMO groups within the MARS data. The more critically ill MARS 1 or 2 group contained more HYPO (52%, 159/308) than NORMO patients, while the less critically ill MARS 3 or 4 group contained fewer HYPO (20%, 34/171) than NORMO patients (p < 0.001). However, the proportion of predicted HYPO among 28-day non-survivors (46%, 53/114) vs. survivors (38%, 140/365) was not significantly different (p = 0.15).
The second study, by Baghela et al., included 345 sepsis patients. We compared patients by in-hospital mortality and found that five of our seven genes, PCSK9, DHCR7, ALOX5, PLTP, and MSMO1 were upregulated (adjusted p < 0.2). ALOX15 was the most downregulated lipid metabolism gene in non-survivors in this cohort, as it was in HYPO patients. These comparisons are displayed in Fig. 4. Finally, we performed a correlation analysis and found that gene expression patterns of HYPO vs. NORMO correlated with MARS 1/2 vs. MARS 3/4 expression patterns (r = 0.335 and p = 0.043), and in-hospital mortality in the study by Baghela et al. (r = 0.737, p < 0.001). Similarly, when comparing by 28-day mortality of patients in our study, these were still correlated with MARS 1/2 vs. 3/4 expression patterns (r = 0.523, p = 0.001), and in-hospital mortality in the study by Baghela et al. (r = 0.552, p < 0.001). Finally, we applied the random forest models to predict the HYPO vs. NORMO patients within the study and examined the difference in the predicted proportion of HYPO patients by in-hospital mortality. We found that the difference was not significant (p = 0.55), with 35% (18/52) of non-survivors classified as HYPO and 29% (86/293) of survivors classified as HYPO, though the overall number of non-survivors was lower than the Scicluna et al. study.
Fig. 4
Comparison of gene expression patterns in external datasets. A Bar plot showing the log2 fold changes of lipid genes for 28-day non-survivors vs. survivors, MARS 1/2 vs. MARS 3/4 (Scicluna et al.), and in-hospital non-survivors vs. survivors (Baghela et al.). Non-expressed lipid genes have been excluded from the corresponding analysis. Colors represent the significance of these genes, determined by the Benjamini-Hochberg-adjusted P value. B Bar plot showing the log2 fold changes of 40 lipid genes for 28-day non-survivors vs. survivors in our study. Seven non-expressed lipid genes have been excluded from the analysis. Colors represent the significance of these genes, determined by the Benjamini-Hochberg-adjusted P value. C Correlation between log2 fold changes from validation sets compared to HYPO vs. NORMO in our study. The x-axis denotes the log2 fold change for HYPO vs. NORMO in our study, and the y-axis shows the log2 fold changes for MARS 1/2 vs. MARS 3/4 (Scicluna et al.) and in-hospital non-survivors vs. survivors (Baghela et al.), separately. D Correlation between log2 fold changes from validation sets compared to 28-day non-survivors vs. survivors in our study. The x-axis denotes the log2 fold change for 28-day non-survivors vs. survivors in our study, and the y-axis shows the log2 fold changes for MARS 1/2 vs. MARS 3/4 (Scicluna et al.) and in-hospital non-survivors vs. survivors (Baghela et al.), separately
留言 (0)