Explanation for the choice of comparators
Participants will be randomized to either receive treatment for CAP per usual care (control group) or to receive treatment for CAP and include a nasal swab with PCR testing to detect the presence of MRSA. Observational studies suggest that there may be a reduction in vancomycin use as the result of using MRSA nasal swab PCR testing to guide antimicrobial stewardship decisions [14,15,16,17,18,19,20,21,22], but this has not been demonstrated in a randomized controlled trial.
Intervention description
Participants randomized to the intervention arm of the study will have a MRSA nasal swab PCR ordered on admission to the MICU, prior to the routine topical nasal decolonization that occurs on all patients admitted to the MICU. For participants enrolled in the control arm, no orders for PCR testing will be placed by the study team. Once the MRSA nasal swab PCR has been completed, the results will be available in the EHR. For the subjects assigned to the intervention group who have a negative MRSA nasal swab PCR result, providers will receive a pager alert which informs them of the negative result and recommends they discontinue vancomycin, if clinically appropriate. The MICU pharmacist will also provide direct education on the test results.
Criteria for discontinuing or modifying allocated interventions
Participants retain autonomy to refuse MRSA nasal swab testing, as with any other clinical procedure. The decision to continue or discontinue vancomycin, or any other antibiotics, will not be dictated by the study, but instead is left solely to the discretion of the medical provider.
Strategies to improve adherence to interventions
Nursing staff in the MICU will receive education on the purpose of the study and the need for collection of MRSA nasal swabs prior to routine topical nasal decolonization. In addition to the direct, instantaneous antimicrobial stewardship guidance to be delivered through a pager alert as outlined above, general education about the use of MRSA nasal swab PCR testing to guide de-escalation of empiric vancomycin will be provided by the MICU pharmacists when a patient with a negative MRSA nasal swab PCR is continued on vancomycin.
Relevant concomitant care permitted or prohibited during the trial
Providers will be allowed to order MRSA nasal swab PCR testing independent of this trial.
Provisions for post-trial care
There are no plans for additional follow-up or post-trial care outside of routine clinical care for the purpose of this trial. Any complications incurred would be those expected as part of routine care, and there is no compensation for participants in the trial.
Outcomes Primary endpoint
Vancomycin-free hours alive: The primary outcome is the expected number of hours out of the first 168 h (7 days) following enrollment in the trial that a patient is alive and not receiving vancomycin, calculated using a proportional odds ratio model. This model is based on a 3-level ordinal status assessed per patient over these 168 h, with the ordinal status levels being alive and not on vancomycin (0), alive and on vancomycin (1), or dead (2).
Secondary endpoint(s)
There are two prespecified secondary outcomes for this trial.
30-day all-cause mortality: Defined as mortality within 30 days with date of study enrollment as day 0.
Time alive off vancomycin: The number of hours out of the 168 h (7 days) following enrollment in the trial that the patient is alive and not receiving vancomycin. Time receiving vancomycin will be defined as the difference from time of administration of the first dose of vancomycin to time of administration of the last dose of vancomycin. If the patient was discharged prior to study day 7 and received vancomycin within 24 h of discharge, then the total duration of vancomycin will be calculated based on the anticipated last day of vancomycin according to the medication reconciliation at the time of discharge or else by using study day 7 as an end point, whichever is sooner.
Exploratory endpoint(s)
There are multiple prespecified exploratory outcomes for this trial, which are defined below.
Hospital length of stay: The difference in days from date of presentation to VUMC to the date of discharge, inclusive of first and last dates.
ICU length of stay: The difference in hours from time of admission to an ICU to transfer out of an ICU (summed if multiple separate transfers to an ICU during the same hospitalization).
Total duration of antibiotic exposure: The difference in days from time of first dose of any oral or intravenous antibiotic to the last dose of antibiotics, inclusive of first and last dates. If the patient was discharged prior to study day 14 and received antibiotics within 24 h of discharge, then the total duration of antibiotics will be calculated based on the anticipated last day of antibiotics at the time of discharge or else by using study day 14 as an end point, whichever is sooner.
Total duration of intravenous antibiotic exposure: The difference in days from time of first dose of any intravenous antibiotic to the last dose of intravenous antibiotics, inclusive of first and last dates. If the patient was discharged prior to study day 14 and had received intravenous antibiotics within 24 h of discharge, then the total duration of intravenous antibiotics will be calculated based on the anticipated last day of intravenous antibiotics at the time of discharge or else by using study day 14 as an end point, whichever is sooner.
Ventilator-free days: The number of days out of the 14 days following enrollment in the trial that the patient is alive and not mechanically ventilated.
Total cost of vancomycin use: The estimated cost of vancomycin administration as a composite of cost of drug, cost of associated laboratory testing, and cost of pharmacy services required to provide dosing.
AKI: An increase in creatinine to ≥ 1.5 times the reference creatinine level or an increase by ≥ 0.3 mg/dL within 14 days of study enrollment [33]. Excludes patients who have end stage renal disease prior to study enrollment.
Receipt of any alternative non-vancomycin anti-MRSA pneumonia antibiotics: Receipt of linezolid or ceftaroline during hospitalization (daptomycin excluded given inappropriate antibiotic selection for pneumonia).
In-hospital all-cause mortality: Mortality at any point during the hospital stay prior to discharge.
Predictive value/concordance with final culture-based results: Among patients with both a MRSA nasal swab PCR and a respiratory culture at any point from admission to 7 days after study enrollment, this outcome is defined as the percentage of patients with a positive MRSA nasal swab PCR who also had any respiratory culture during the first 7 days after study enrollment that was positive for MRSA (positive predictive value) and the percentage of patients with a negative MRSA nasal swab PCR who also had any respiratory culture during the first 7 days after study enrollment that was negative for MRSA, regardless of whether another pathogen was detected or not (negative predictive value).
Implementation endpoints
Time to result: Time from collection of swab to results being available in EHR.
Fidelity endpoints
Fidelity of obtaining MRSA nasal swab: Percentage of patients randomized to intervention arm who have a MRSA nasal swab collected.
Fidelity of running and reporting PCR results: Percentage of patients who have a MRSA nasal swab collected who have PCR testing performed and results reported in the EHR.
Fidelity of paging alert to team: Percentage of patients in the intervention arm with a negative MRSA nasal swab PCR test result who have pager alerts sent to their primary provider.
Participant timeline
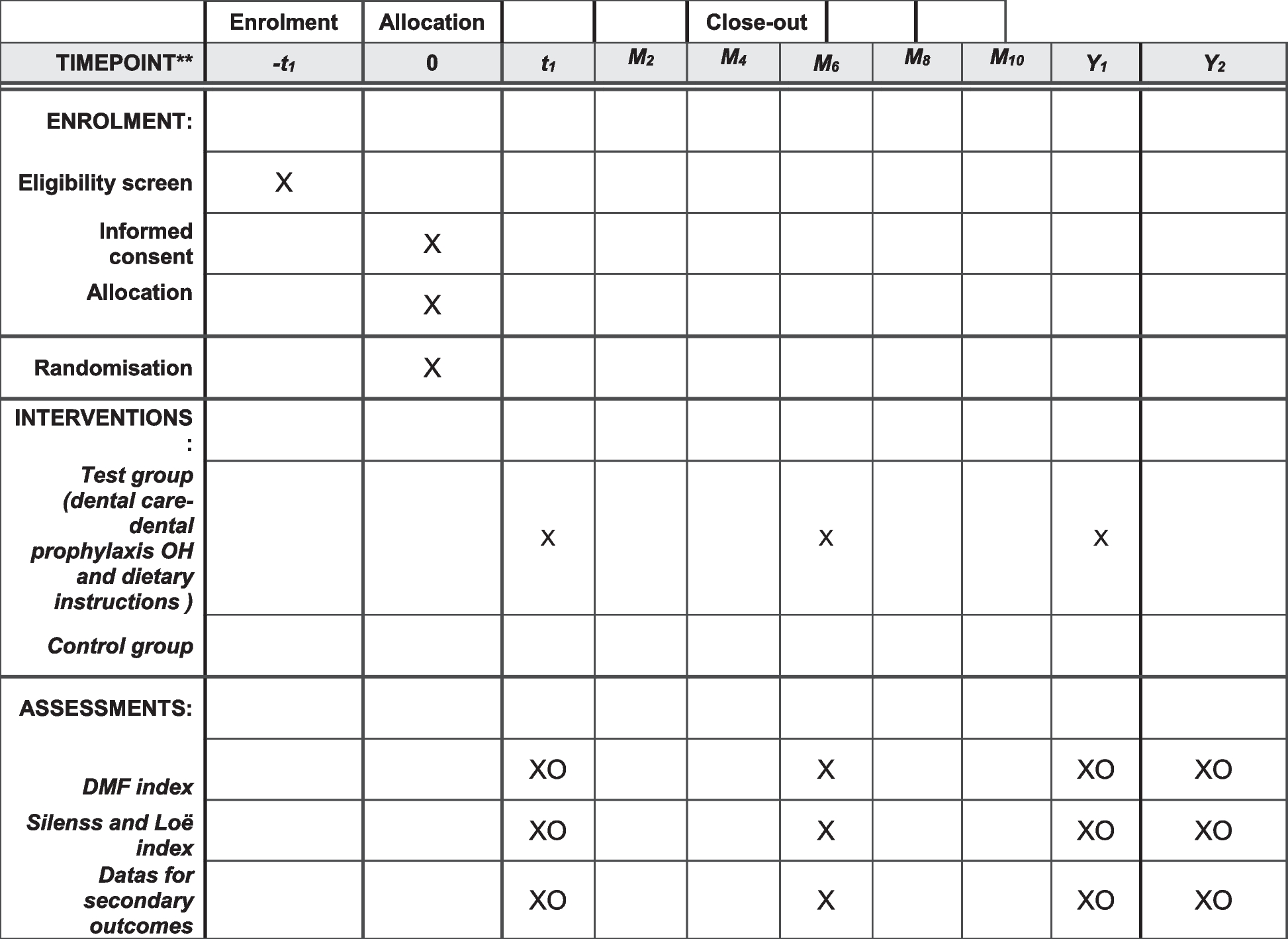
A participant timeline is shown in Table 1.
Table 1 Standard Protocol Items: Recommendations for Interventional TrialsSample size
The method used for sample size estimation is based on a traditional univariate proportional odds model. The actual primary analysis is based on a longitudinal proportional odds model that makes use of hourly patient status. For the purposes of this study, a 24-h reduction in vancomycin use is considered clinically meaningful.
To overcome challenges with mortality, which is estimated at 22% within 8 days [34], the primary outcome, “vancomycin-free hours alive,” is defined as the number of hours alive and free of the use of vancomycin within the first 7 days of study enrollment. This is not a quantity that is calculated on raw data because of deaths but is derived from the longitudinal model described below. The result is summarized as a treatment difference in mean vancomycin-free hours alive for specific covariate settings (p values are the same for all covariate settings since treatment is not allowed to interact with covariates). The result will also be summarized by an OR for the hour-to-hour state transitions, from the proportional odds longitudinal model.
In those who do not die, it was estimated from preliminary data from the VUMC MICU that the relative frequencies for all possible outcomes will be equal to 0.023, 0.008, 0.019, 0.027, 0.095, 0.125, 0.224, and 0.262 (for 0 to 7 vancomycin-free days). Given this distribution, and an assumption of 22% mortality [34], an overall 24-h increase in mean “vancomycin-free hours alive” would be associated with a common OR for a univariate proportional odds logistic model of about 2.2. To detect this difference with 90% power and a two-sided alpha level of 0.05 would require about 106 subjects per study group.
Recruitment
Patients will be automatically enrolled and randomized either upon transfer to the MICU with an order for “pharmacy consult for vancomycin dosing” already in place if a respiratory culture has been ordered, or when the indication for vancomycin or for “pharmacy consult for vancomycin dosing” is “respiratory infection.” If an order for vancomycin or a “pharmacy consult for vancomycin dosing” order is placed (within 24 h of admission to the unit) for a patient located in the MICU, they will also be automatically enrolled if a respiratory culture has been ordered, or when the indication for vancomycin or for “pharmacy consult for vancomycin dosing” is “respiratory infection.”



留言 (0)