
記住我
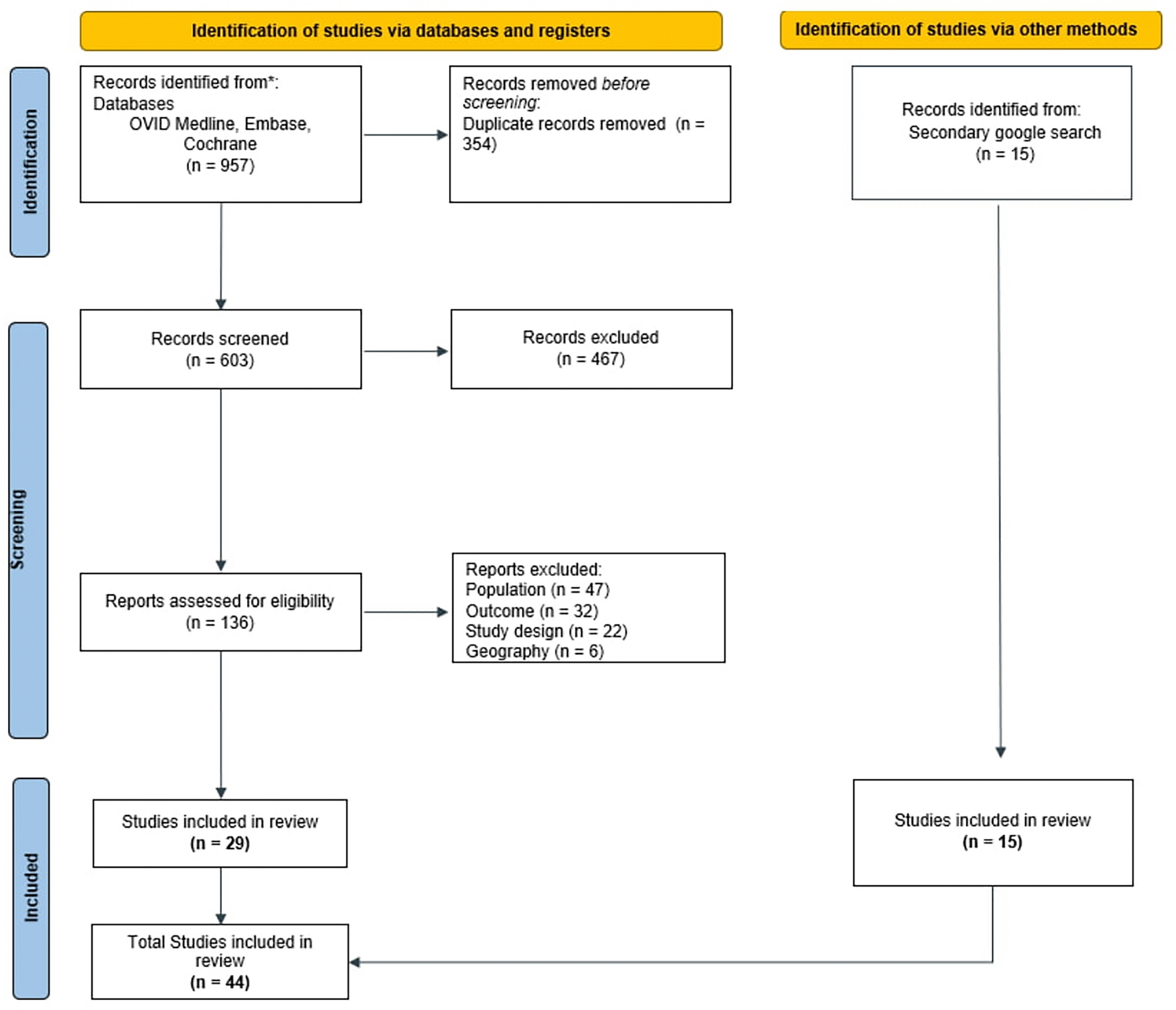

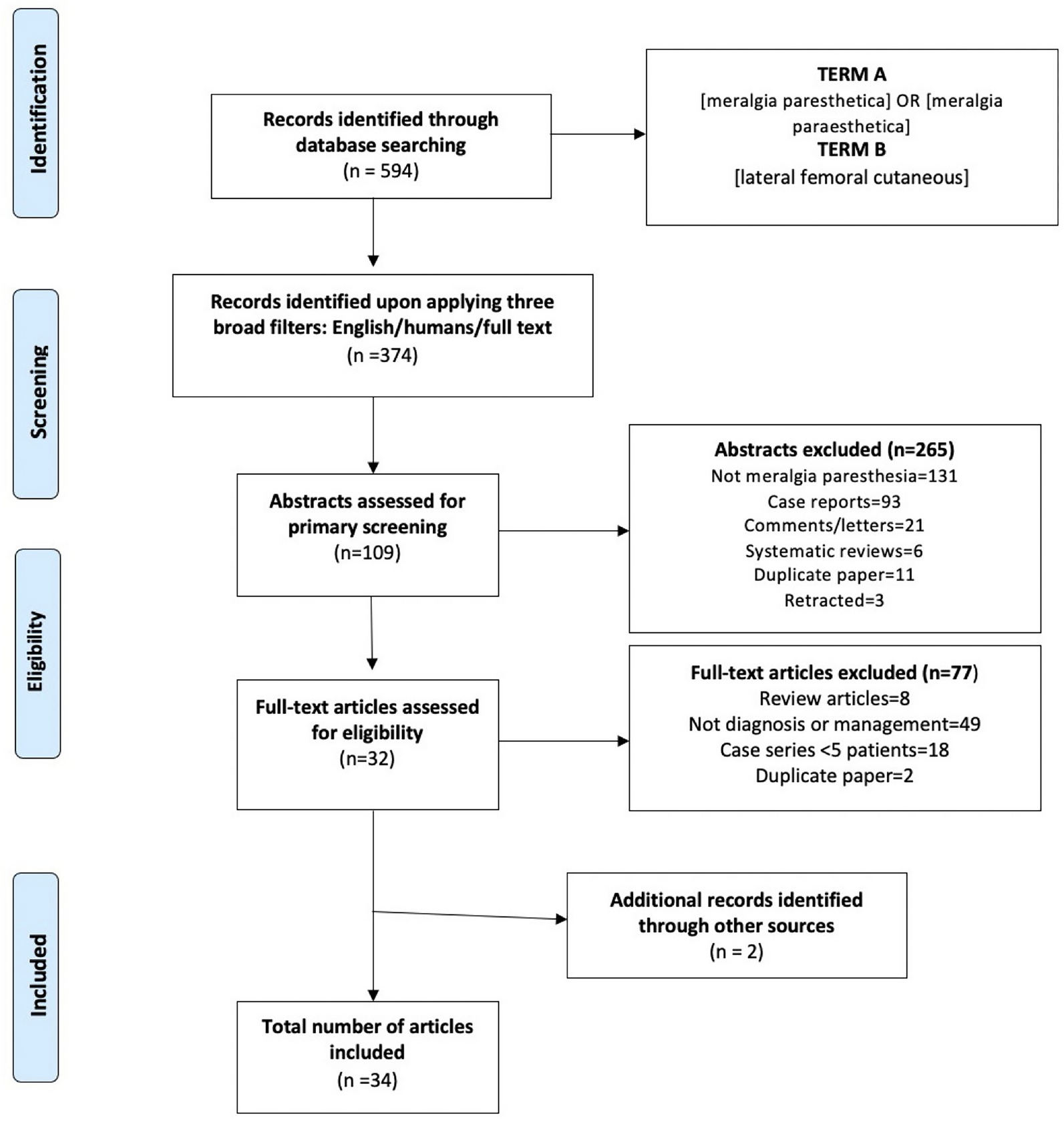
The SLR identified 957 articles from the 3 databases. After removing 354 duplicate publications, 603 articles were screened for title/abstract eligibility. Following screening, 467 articles were excluded, and 136 were retrieved for full-text assessment. Based on further exclusion of articles that did not meet the eligibility criteria, 29 studies were included in the SLR report for data extraction. Additionally, 13 records were identified from a secondary search, leading to a total of 42 articles being included in the SLR. The PRISMA diagram (Fig. 1) presents the details of the study selection.
Fig. 1 Patient Epidemiology
Patient EpidemiologyThe SLR encompassed 14 studies focused on patient epidemiology for the ME region. Of these, two studies from Egypt, six studies from the Kingdom of Saudi Arabia (KSA), two from Iran, and one each from Jordan, Qatar, Iraq, and Kuwait were included.
The estimated prevalence of migraine in the general population in the ME in 2020 was 2.6–32.0% [5]. In Egypt, the prevalence among individuals aged 18–40 years ranged from 4.8 to 10.5% between 2009 and 2012 [20, 21]. A pronounced country-specific variation was noted in the prevalence: 14–27.6% in Iran [22, 23], 5.0–37.2% in the KSA [24,25,26,27,28], 23.1% in Kuwait [29], 7.7% in Jordan [30], and 26.3% in Iraq [31]. The fastest decrease in the incidence was noted in Qatar from 1990 to 2019 [32]. Evidently, migraine prevalence was highest among young adults aged 18–30 years, indicating a significant impact on this patient group [20, 29]. Furthermore, a gender disparity was observed, with women exhibiting a higher prevalence than men, at a ratio of 2–2.5:1, with the highest difference observed in the patient population from the KSA [20, 25, 27, 29]. Table 1 provides the details of the studies included in the SLR for patient epidemiology.
Table 1 Summary of studies related to epidemiology of migraines and patient characteristics specific to Middle East regionThe patient prevalence in the ME region was similar to that in the US, where it ranged from 11.7 to 14.7%, with a higher prevalence noted among women [33]. Apart from these studies, a recent cross-sectional population-based study carried out in Morocco with 3474 participants found that the prevalence of migraines was 30.8%, while the prevalence of tension-type headaches was 32.1% [34]. There is clearly an unmet need for more region-specific epidemiological studies to better understand the prevalence and impact of migraine across different demographics in the ME region. This will help tailor public health strategies and resource allocation.
Patient CharacteristicsFor the evaluation of patient attributes, the SLR captured eight studies. Most were conducted in the KSA [3], while Iran, Jordan, Egypt, Sudan, and Kuwait had one study each.
The mean patient age across the studies in the ME region ranged from 27 to 37.5 years, suggesting that migraines primarily affect individuals in their early to mid-adulthood [21, 23, 25, 29, 30, 35]. The results from the SLR are consistent with a real-world study in the US [36] and a retrospective database analysis in Japan [37], which reported the mean ages of patients with migraine at 40 and 38.8 years, respectively.
In terms of patient characteristics, most patients with migraine in the KSA were married (59.6%), had a graduate-level education (60.8%), were employed (52.8%), and were smokers (16.8%) [35]. Interestingly, in Jordan, most patients were single (70.7%) and university students (49.2%) [30]. A slight difference was observed in Egypt, with 69.7% of Egyptian patients belonging to a lower socioeconomic stratum [21]. The results obtained from the study in the KSA and Jordan are in alignment with the study conducted in Malaysia, where most patients were single (52.3%), as in Jordan, with tertiary-level education (70.5%) as in the KSA [38]. Table 1 provides the details of the studies included in the SLR for patient characteristics.
Gender disparity was noted in patient characteristics across the ME region, with a higher prevalence of migraine among women (KSA: 83.2% women vs. 16.8% men; Kuwait: 31.7% women vs. 14.8% men; Iran: 36.7% female vs. 21.6% male; Egypt: 24.8% women vs. 15.2% men; Jordan: 36.7% women vs. 21.6% men). The highest gender difference was observed in the KSA among the countries of interest [21, 23, 27, 29, 30, 35]. In a cross-sectional retrospective analysis conducted in the US, a high prevalence of menstrual migraine was recorded in female patients with migraine (overall: 31.0%, pre-menopausal female patients: 52.5%). This suggests a potential hormonal influence on migraine occurrence among women [39]. Additionally, in a case-control study conducted in Sudan that evaluated pregnant women with pre-eclampsia, it was observed that pregnant women with a history of migraine had higher odds of pre-eclampsia than women without migraine [40]. A meta-analysis conducted among 187,328 pregnant women with a migraine diagnosis from 2000 to 2018 also demonstrated that migraine was associated with increased odds of pre-eclampsia, peripartum mental illness, and preterm birth [41]. Therefore, these findings emphasize the need for a gender-specific approach to understanding and managing migraines, considering the higher prevalence in women. Further research is needed to explore the sociodemographic factors influencing migraine characteristics in the ME region. This includes understanding the impact of socioeconomic status, education, and employment on migraine prevalence and management.
Prodromal Symptoms (Interictal Burden) and Psychosocial EffectsIn total, seven studies were included regarding the comorbidity and psychosocial analysis, of which three were from the KSA, two from Egypt, and one each from Iran and the United Arab Emirates (UAE).
The most common symptoms observed among patients with migraine in the ME region were photophobia (88.5%), followed by nausea (58.9%) and lacrimation (53.4%). Notably, a significant proportion of patients also experienced chronic sinusitis (37%) and depression (26.1%) [21, 25]. In a study conducted in the KSA, prodromal symptoms, which often serve as a warning sign of impending migraine attacks, were observed, with flashes recorded in 42.8% of cases [25]. In addition to these symptoms, it is pertinent to note that migraine is often accompanied by other health conditions, most of which are attributable to its complex physiological mechanism. Patients with migraine experience other health conditions, including anxiety, chronic sinusitis, depression, epilepsy, stroke, multiple sclerosis, systemic lupus erythematosus, heartburn, cardiovascular diseases, hypotension, irritable bowel syndrome, dyspepsia, nonalcoholic fatty liver disease, and cholelithiasis [25, 42,43,44,45]. In a survey conducted in the UAE among patients with neurological disorders (75 patients with migraine included), 39% experienced depressive symptoms and 34% had anxiety [46]. In a recent retrospective e-claims database study from the UAE, 13.4% of patients with migraines reported cardiovascular comorbidities during the study period between 2014 and 2022 [47]. In a cross-sectional study conducted in Egypt among patients aged ≥ 18 years, it was noted that women with menstrual migraines had a significantly higher frequency of generalized anxiety disorder, panic attacks, and restless leg syndrome than those with non-menstrual migraines [42]. Table 2 presents the details of the studies included in the SLR for comorbidities and psychosocial effects.
Table 2 Summary of studies associated with comorbidities, psychological effects, and triggers related to migraines in Middle East regionThe comorbidities experienced globally are in alignment with those identified in the ME region. The commonly reported comorbidities in patients with migraine in the US and Japan, as determined in the patient survey and cross-sectional study, respectively, included anxiety, gastrointestinal (GI) issues, angina, depression, epilepsy, and hypertension [9, 48, 49]. Thus, these observations underscore the complex interplay between migraines and various other health conditions, highlighting the need for comprehensive health care strategies that address these co-existing conditions to improve patient-related outcomes. There is clearly an unmet need for integrated health care approaches that address both migraine and its comorbid conditions. Future studies should focus on the psychosocial impact of migraines and the development of holistic treatment strategies.
Quality-of-Life/Humanistic and Productivity BurdenFor the QoL and humanistic burden, a total of 13 articles were included (eight from the KSA, three from Iran, one from Egypt, and one global study focusing on the ME).
The studies captured by the SLR demonstrated moderate-to-severe disability, based on Migraine Disability Assessment (MIDAS) scores in the restrictive, preventive, and emotional domains. MIDAS is an organized, standard questionnaire to assess the level of migraine pain and determines the severity of disability in affected individuals. Lower scores indicate no disability, while high scores represent severe disability [50]. It was also observed that patients with episodic headaches had lower MIDAS scores than those with chronic headaches who had elevated scores. Notedly, patients who had fewer frequent migraine attacks exhibited better QoL [20, 35, 50,51,52,53]. An elevated MIDAS score and more frequent migraine attacks had a positive correlation with disability severity, implying impairment of daily activities [13]. Patients with migraines struggle with social isolation and physical limitations, experience embarrassment, unkindness, and discomfort from others, and they blame themselves for the illness, leading to exacerbated emotional distress. This often leads to negativity among patients, causing shame, guilt, depression, and low self-esteem [54]. Furthermore, daily activities, preventive behaviors, and the emotional well-being of patients remain affected. This profound impact on patients underscores the significance of effective management strategies to reduce the frequency of migraine attacks. Table 3 provides the details of the studies included in the SLR for the humanistic burden in migraine.
Table 3 Summary of studies related to humanistic burden of migraine specific to Middle East regionSimilar trends in the humanistic burden were observed between the ME region and other global counterparts. In a randomized clinical trial conducted in the US, 90% of patients reported a negative impact on overall life, making life more difficult and causing disability during migraine attacks. Reportedly, 52% and 14% of patients saw an impact on emotional health and cognitive function, respectively. Around 68% experienced an impact on work productivity as well as family and social life [55]. In Spain, migraines led to productivity losses at work and impairment of daily activity at higher headache frequencies [56]. In a cross-sectional survey conducted in five countries in Europe, patients with a higher monthly headache frequency experienced higher activity impairment and more frequent visits to health care providers [57]. In Turkey, based on the hospital anxiety depression scale, illness perception questionnaire, and Quality-of-Life Short Form-36, headache severity and duration were higher among patients with migraine. Social functionality and pain scores were lower among patients with migraine [58]. One other US study among adult patients with high monthly migraine frequency reported that 46% of the patients felt left out of things, 38% felt embarrassed because of physical limitations, and 34% expressed resentment over others feeling that it was their fault that they had migraines [54]. At the workplace, patients experienced a lack of understanding of their illness among their peers, impaired relationships, and the burdening of colleagues with headaches. Migraines also resulted in a loss of energy and an inability to concentrate at work, resulting in a loss of productivity [59]. The negative connotation associated with migraines had a higher impact on disease outcomes, psychiatric symptoms, MIDAS severe disability, and the emotional quotient of QoL [60].
Occupational burden is another important aspect of functional impairment due to migraine, leading to productivity loss. Absenteeism refers to complete absence from work due to migraine, while presenteeism is a condition wherein the employee continues to work even with migraine [61]. Working patients were likely to demonstrate poor QoL in the KSA, as established from a cross-sectional study [53]. Migraine led to absenteeism at work and low work productivity, highlighting its occupational burden. In a study conducted in the US, 68% of migraines occurring during the workday resulted in absenteeism, presenteeism, or both (total productivity loss) [62]. Caregiver burden is another neglected aspect related to migraine. A narrative analysis study involving patients, caregivers, and clinicians from Italy reported that nearly 86% of caregivers felt migraines negatively impacted their QoL in terms of loss of time and energy, with 14% confirming the experience to be difficult and challenging [63].
A potential gender disparity has also been evidenced in the impact of migraine. In studies conducted in the KSA (cross-sectional studies and Web-based survey), women exhibited a significant relationship between migraine-associated disability and patients' emotional function regarding QoL. However, men demonstrated better QoL parameter values [27, 35, 51]. Similar outcomes were reported in Malaysia, where women with migraine reported significantly lower QoL with severe and frequent disability compared with healthy controls [64]. Therefore, it is evident that migraines significantly impact the QoL, affecting emotional health, cognitive function, work productivity, and social life across various global regions, underscoring the need for effective management strategies to mitigate this burden. These published reports show an unmet need for more region-specific studies to understand the humanistic and productivity burden of migraines in the ME region. Additionally, developing targeted interventions to address these burdens can significantly improve the QoL for patients with migraine.
BiomarkersThe SLR captured a total of five articles, with two from Egypt and one each from the KSA, Kuwait, and Asia. Despite the high prevalence of migraine in the ME region, studies related to biomarkers associated with migraine are limited within the region. Biomarkers are probably beneficial in migraine diagnosis, determining the response of any specific treatment, and may have applicability in developing newer therapies, particularly precision medicine [65]. Global literature on pre-clinical and clinical biomarker studies has demonstrated the role of biomarkers such as neuropeptides CGRP, pituitary adenylate cyclase-activating polypeptide (PACAP), classic neurotransmitters (glutamate), inflammatory mediators (cytokines), endocannabinoids, endothelin-1 (ET-1), and tryptophan in the pathophysiology of migraine [65]. There is a significant lack of data on biomarkers within the ME region. Future studies should focus on identifying and validating biomarkers to enhance diagnostic accuracy and treatment efficacy for patients with migraine in this region.
TriggersIn a population-based cross-sectional study in Egypt, the common precipitating factors for migraine attacks were observed to be glair (63.10%), family troubles (53.02%), vigorous exercise (26.41%), and fasting (25.81%). These factors highlight the multifactorial nature of migraine triggers [
留言 (0)