
記住我

A contemporary, nationally representative database was used for the analysis (STATinMED’s RWD Insights). This data was publicly available and aggregated and included claims data from approximately 80% of the US health care system (Medicare, Medicare Advantage, Medicaid, and commercial insurances). This data is sourced directly from claims clearing houses, which are responsible for managing claims transactions as they go between payers and providers. Data were de-identified, and data use complied with the requirements of the Health Insurance Portability and Accountability Act (HIPAA) for the privacy and security of protected health information. Since this study used retrospective data, initially available in the public and anonymized the study did not meet Health and Human Service Services definition as human research (as defined in 45 CFR 46.102) and was exempt from IRB review.
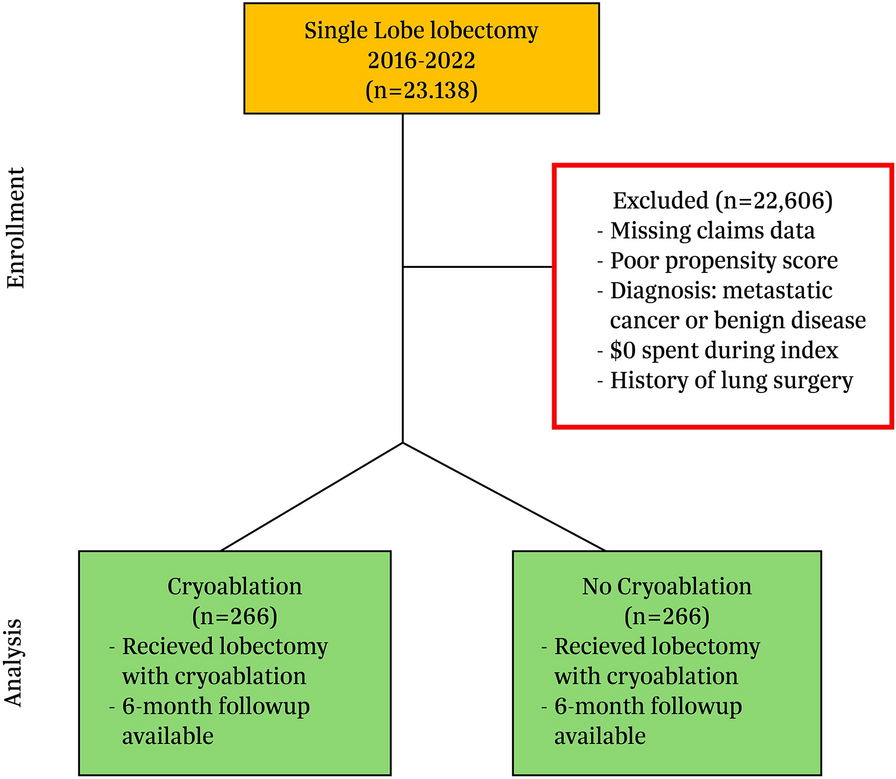
Patient SelectionPatients aged 18 years or older undergoing single surgical lobectomy between January 1, 2016 and December 31, 2022 were selected for the study (Fig. 1). Patients with open, video-assisted thoracic surgery (VATS), or robotic-assisted thoracic (RATS) approach were included. Patients in the cryoablation group had International Classification of Diseases, Tenth Revision, Procedure Classification System (ICD-10-PCS) procedure code (01580ZZ or 01584ZZ) during the index visit. The cryoablation procedure is performed as a distinct ancillary ablation procedure (− 50 to − 70 °C for 120 s per level) at multiple levels using the AtriCure CryoICE cryoablation system (AtriCure, Inc; Mason, OH) (Fig. 2). Under direct visualization the surgeon identifies the intercostal nerves and ablates the intercostal spaces, usually five levels before lobectomy. In the authors hands, cryoablation typically requires 8–12 min operative time to administer and is considered ancillary to the planned primary lobectomy procedure. The cryoablation intervention was added to non-standardized standard of care (SOC; epidural, regional blocks, opioids, non-opioids, etc.) for postsurgical pain management at each institution and compared to those undergoing SOC without cryoablation.
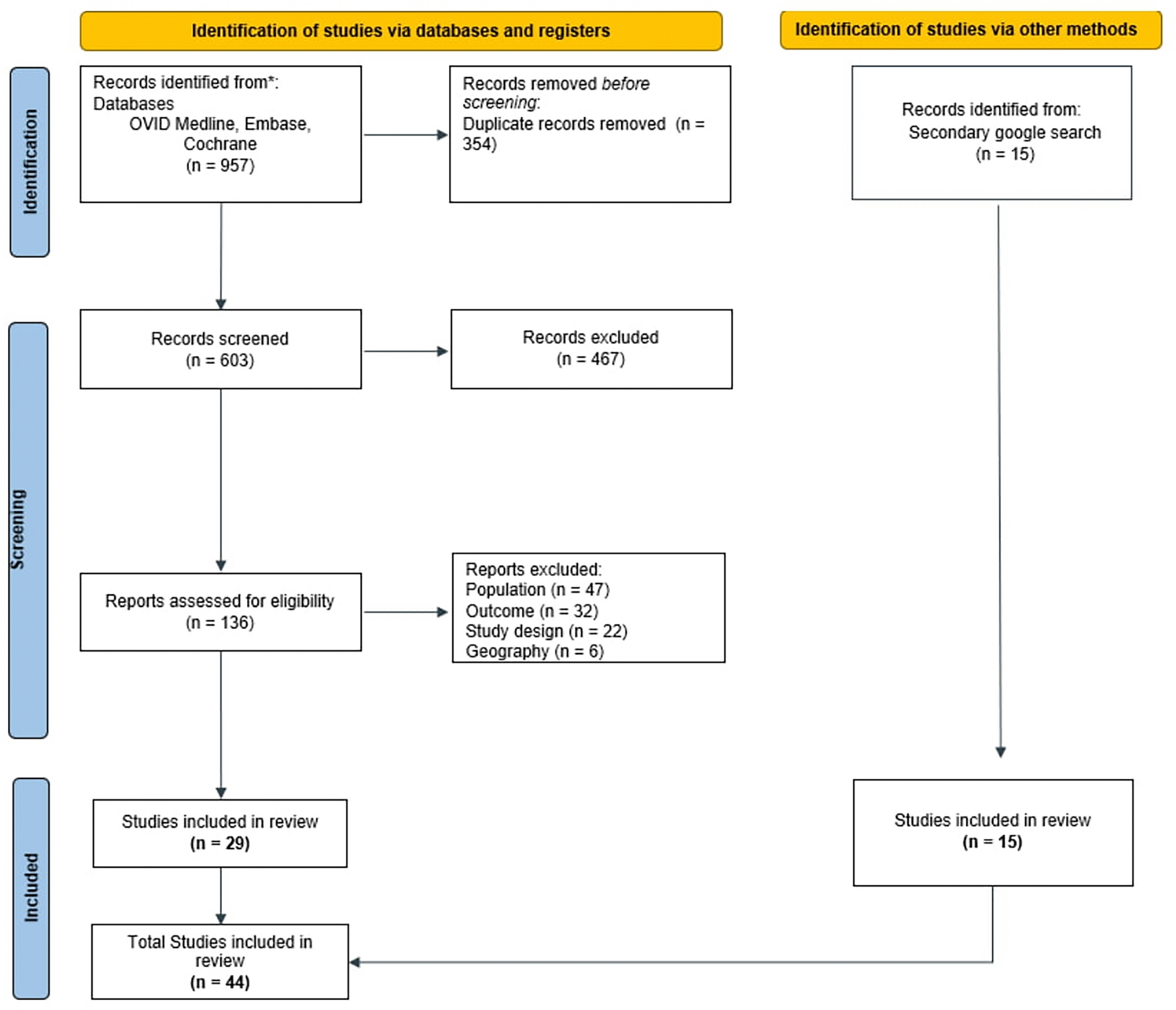
Fig. 1
CONSORT diagram. Adult patients who had lobectomy for lung cancer performed between January 1, 2016 and December 31, 2022 were included. Patients with missing claims data preoperatively and during follow-up, those with metastatic cancer or infectious etiology, or $0 spent for index procedure were excluded. The final matched cohort included 266 patients in both groups
Fig. 2
Cryoablation of intercostal nerve during surgical lobectomy
Patients had continuous capture of medical and pharmacy benefits for the 12-month pre and at least 6 months after the index date. Six months postoperatively was chosen given the importance to assess continued use of opioids following surgery. Exclusion criteria included prior lung surgery such as lobectomy, pneumonectomy, or sublobar resection (segmentectomy and wedge resection) in the 12 months prior to index. Other exclusion criteria included lung resection for metastatic disease, benign disease, or $0 spent on the index visit.
Patient DemographicsPatient demographic characteristics and procedure variables were recorded at the index date and included age, gender, lobe resected, geographic area, and insurance type. Comorbidities of interest were identified using International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) present in claims. Key comorbid conditions included presurgery atrial fibrillation, congestive heart failure, chronic obstructive pulmonary disease, hypertension, smoking status, opioid use, and chemotherapy status.
Clinical and Economic OutcomesThe primary study endpoints were average length of stay (ALOS), postdischarge resource use, hospital readmissions, emergency department (ED) visits, and hospital outpatient and pharmacy costs over time. Opioid use and dosage were estimated as morphine milligram equivalents (MME) from prescriptions filled (Supplemental Methods). Secondary endpoints included safety variables such as pneumonia, pneumothorax, prolonged air leak, and acute respiratory failure.
Medicare cost reports from claims submissions using cost-to-charge ratios (CCR) were used to estimate average hospital costs. Costs included both direct and indirect costs and included various cost centers (operating room, pharmacy, supplies, etc.). CCR are standard ways in which US Medicare reports costs and utilization. Summed costs over time included total healthcare costs, inpatient services, outpatient services, and total outpatient pharmacy costs (included National Drug Code, NDC) claims only. Physician fees were not included in the cost analysis, as they usually represent less than 10% of hospital reimbursement.
Propensity Matching and Statistical AnalysisPropensity score matching (PSM) was used to control patient baseline differences. PSM reduces the effects of bias and confounding variables by removing confounding factors between groups and increasing comparability between the groups [13]. Variables used in the PSM logistical regression included age, gender, prior opioid use status, surgical approach, and lobe resected. Patients who underwent lobectomy with and without cryoablation were matched using the nearest neighbor matching method, a caliper width of 0.1, and no replacement resulting in a 1:1 matched sample reducing standardized differences to less than 0.1 after matching. After matching, comparisons were described using proportions for categorical variables and means with standard divisions for continuous variables. Differences between groups were tested with the chi-square test for categorical variables and Student t test for continuous variables. To minimize the effect of outliers on our estimates we employed Winsorization at the 97.5th and 2.5th percentiles when outliers were identified. For patients with opioid dosage above the 97.5th percentile the values were set to the 97.5th percentile level. Similarly, for those below the 2.5th percentile, the values were set to the 2.5th percentile level. A p value less than 0.05 was considered significant. Analyses were performed using R Version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria).
留言 (0)