
記住我
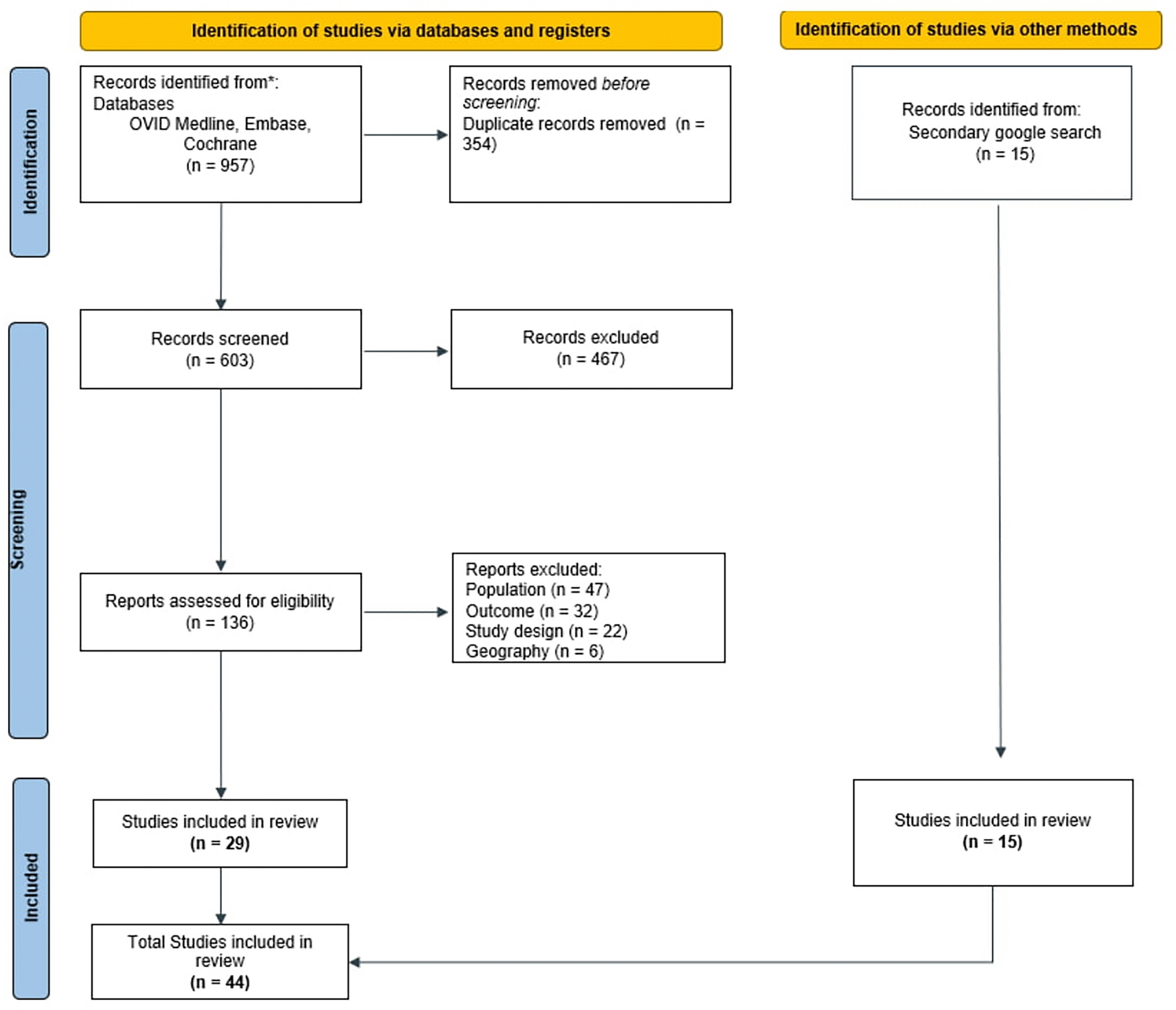

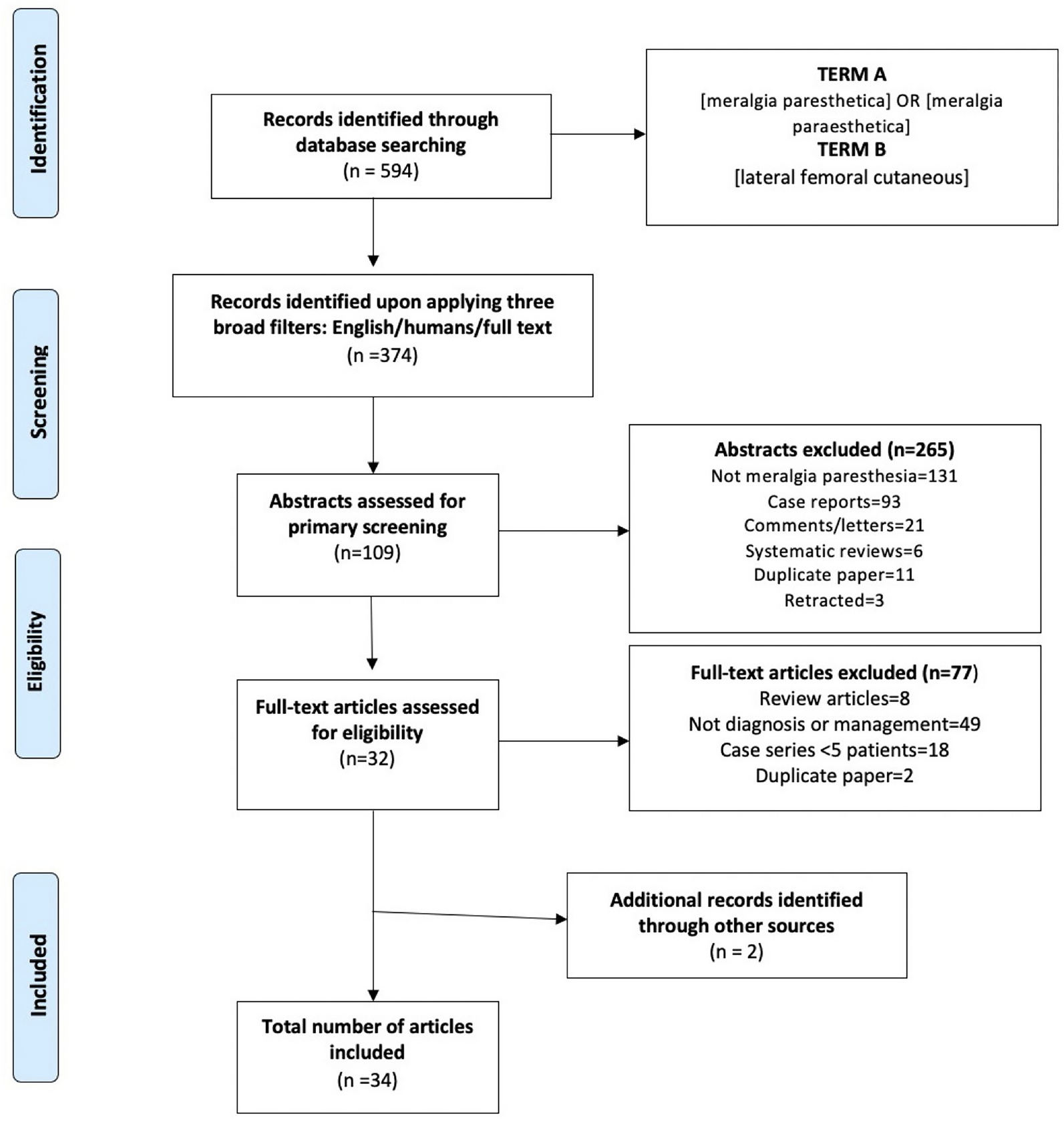
The above-mentioned literature search strategy returned 594 articles. Following a two-stage screening process, 32 articles were deemed eligible for inclusion. Two further articles were found via reference searching leaving a total of 34 articles for review [8, 10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42]. Figure 1 illustrates the study selection process.
Fig. 1
PRISMA chart displaying screening process
Diagnosis of MPOf the 11 papers that discuss diagnosis, 5 [10, 13,14,15,16] focused on imaging and 6 [8, 17,18,19,20,21] focused on electrophysiology.
Bedside TestsThree bedside tests have been described in the literature: the pelvic compression test, neurodynamic testing and the Tinel test. These tests are often incorporated into research articles and there exists little literature exploring the effectiveness of these tests or comparing them. This is a gap in the literature that should be looked at filling in future works.
The pelvic compression test (Fig. 2) was first described by Nouraei et al. in 2007 [36]. The patient is positioned on their side with their symptomatic side facing upwards. The examiner applies a downwards, compression force to the pelvis and maintains pressure for 45 s. If the patient reports an alleviation of symptoms, the test is considered to be positive. This test is based on the idea that the LFCN is compressed by the inguinal ligament and that a downward force to the innominate will relax the ligament and temporarily alleviate the patient's symptoms.
Fig. 2
Neurodynamic testing (Fig. 3) was described by Butler [43] wherein the patient is lying on their side with the symptomatic side facing upwards and the bottom knee bent. The examiner stabilises the pelvis with their top hand and grasps the lower extremity at the knee with their bottom hand. The examiner then bends the knee and adducts the hip in order to elicit tension in the LFCN. A positive test would be the reproduction of the patient's neurologic symptoms versus feeling tension in the soft-tissue structures of the hip which would be considered negative.
Fig. 3
While the Tinel test is largely regarded to be diagnostic for carpal tunnel syndrome, Parmer reported the possibility of eliciting the Tinel test on the LFCN in patients with suspected MP [44]. In this test, the patient is lain supine and the examiner taps on the LFCN just medially to the anterior superior iliac spine (Fig. 4). A reproduction of symptoms indicates a positive test.
Fig. 4 ImagingUltrasound (US)
ImagingUltrasound (US)Ultrasound (US) as a diagnostic tool was assessed in three papers [10, 13, 14]. These papers looked at producing diagnostic criteria when analysing potentially pathological LFCNs, focusing on cross-sectional areas and nerve diameters. All three papers reported a significant difference between cross-sectional areas (CSAs) in pathological versus non-pathological nerves. Suh et al. reported a median CSA of 11 mm2 (range 5–28 mm2) in pathological LFCNs and a median CSA of 3 mm2 (range 2–6 mm2) in healthy LFCNs, thus suggesting a significant difference in CSA between pathological and non-pathological LFCN’s (p < 0.001). Powell et al. reported a mean CSA of 9 mm2 (range 3–25 mm2) in pathological LFCNs and a mean CSA of 3 mm2 (range 1–9 mm2) in healthy LFCNs, thus also suggesting a significant difference between pathological and healthy LFCN’s (p < 0.01). Both papers suggested a cut-off value of CSA > 5 mm2 being diagnostic for MP, with Powell et al. reporting a 87% sensitivity and 90% specificity and Suh et al. reporting 95.7% sensitivity and 95.5% specificity at this cut-off.
Aravidakannan and Wilder-Smith looked at CSA but also looked at the nerve diameter using an 8- to 13-MHZ linear-array transducer. They reported a mean CSA of 4 mm2 (range 2–5 mm2) in known MP nerves and a mean CSA of 2 mm2 (range 1–3 mm2) in healthy nerves, thus reporting a significant difference in CSA’s between healthy and pathological nerves (p < 0.05). When looking at mean nerve diameter in healthy and MP confirmed nerves, they reported a mean diameter of 0.40 cm (range 0.37–0.42 cm) in pathological nerves and a mean diameter of 0.21 cm (0.16–0.30 cm) in healthy LFCNs. Again, there was a significant difference between healthy and pathological nerves (p < 0.05).
Two studies [10, 16] looked at the effectiveness of US imaging in identifying the LFCN as well as pathology in the LFCN. Lee et al. [16] used high-resolution (15–18 MHz) linear US transducers in 136 patients known to have pathology and reported that, in 131 patients, the LFCN was able to be visualised, a 97% success rate. However, of the 136 known pathological nerves, only 83 were identifiable through US, a 49% success rate. Identifiable pathology included perineural scarring, impingement, neuroma and nerve thickening. Powell et al. [10] imaged the LFCN in 50 patients using a 5- to 12-MHz linear transducer. Of the 50 patients with suspected MP, the LFCN was visible in 45 patients, a 90% success rate. Of the 50 known nerves with MP, US found abnormalities suggestive of MP in 35 cases, a 70% success rate.
Magnetic Resonance Imaging (MRI)MRI imaging was assessed in three papers (Lee et al. [16], Powell et al. [10] and Chhabra et al. [15]). Lee et al. [16] performed MRI in 51 patients and reported a 60% accuracy in identifying the LFCN. Of the 51 known pathological nerves, pathology was identifiable in 15 nerves, a 29% accuracy. Identified pathologies included inflammation, compression and neuromas. Powell et al. [10] performed MRI in 16 patients with suspected MP and identified positive indicators of MP pathology in 4 nerves, a 25% accuracy.
Chhabra et al. [15] assessed MRI in 11 patients and reported a 100% accuracy in identifying the LFCN and a 90% accuracy in identifying pathological LFCNs. They further go on to suggest that MRI has a 71% sensitivity and 94% specificity in identifying LFCN pathology indicative of MP. It should be noted that the paper by Chhabra et al. uses a 3 Tesla MRI, while the other two papers do not report metrics on strength of the MRI machine (Table 1).
Table 1 Characteristics of studies using imaging techniques (ultrasound or MRI) to diagnose meralgia parestheticaElectrophysiologyBoth somatosensory evoked potentials (SSEP) and sensory conduction studies (SCS) have been researched for their usefulness in diagnosing MP. SSEP are recorded through surface electrodes placed at the scalp after a continuous electrical stimulation is applied at a peripheral nerve. Among others, they measure the time of conduction from peripheral to central nervous system. During SCS, the sensory nerve action potential (SNAP) is recorded from surface electrodes at the area of innervation when an electrical stimulus is applied at a nerve. Based on the distance between stimulation and recording one can calculate the nerve conduction velocity (NCV).
SCSSpevak and Prevec [19] used SCS to assess MP in 13 patients (total of 14 nerves as 1 was bilateral). They assessed the use of NCV and SNAP amplitude and reported on the scope of using side to side ratio (ssRATIO/ L–R difference) on NCV as a more accurate metric for diagnosing MP, instead of slowed NCV alone. They note that SNAP measurements were possible in 9/14 nerves (8/13 patients). They reported that a normal NCV of 62.3 ± 5.5 m/s versus a pathological NCV of 51.3 m/s. When looking at ssRATIO difference in NCV, they noted 7/8 patients having a significant difference between healthy and MP nerves, giving an 87.5% accuracy. It should be noted that, while Spevak and Prevec suggested an ssRATIO difference in NCV to be a useful tool for diagnosing MP with SCS, the paper does not specify an exact diagnostic cut-off. Overall, they concluded that absolute slowing of the NCV as well as L–R differences in NCV are better diagnostic tools for MP compared to SNAP amplitude.
The work by Spevak and Prevec was built on by Seror in 1999 [8]. Seror examined 30 patients and looked at an ssRATIO amplitude differences instead of NCV difference as well as NCV and SNAP amplitude. Seror was only able to record SNAP in 17/30 patients. He reported that the ssRATIO for amplitude was abnormal in 100% of patients with suspected MP, and that this metric had a 98.8% sensitivity. SNAP amplitudes between patients with MP and healthy were significantly different, with mean pathological nerve SNAP amplitude of 1.5 ± 2.1 μV and mean healthy nerve SNAP amplitudes of 16 ± 7 μV (p < 0.05). Seror also reported no significant difference in NCV between healthy and MP suspected nerves, with mean healthy NCV of 60 ± 5.3 m/s and mean pathological NCV of 57 ± 4.4 m/s (p > 0.05). Unlike Spevak, Seror did describe a diagnostic value for both SNAP amplitude and ssRATIO, with a SNAP amplitude < 3 μV and a ssRATIO > 2.3 being diagnostic.
Seror and Seror in 2006 then explored the use of SCS in diagnosing MP, with a particular focus on assessing the SNAP amplitude. They assessed 120 patients (131 nerves, 11 bilateral patients) with clinically probable MP. Similarly to Seror’s work in 1999, they found no significant difference in the NCV between pathological and healthy nerves, with the MP nerve groups having a mean NCV of 55.6 ± 6 m/s and the control group having mean NCV of 60 ± 5.3 m/s (p > 0.05). They did report a significant difference between the SNAP amplitudes between MP and healthy nerves, with MP nerves having a mean SNAP amplitude of 2.0 ± 2.5 μV and healthy nerves having a mean SNAP amplitude of 16.1 ± 7.2 μV (p < 0.0001). They determined that the two cut-off values that were diagnostic for MP were the SNAP amplitude < 3 μV and the ssRATIO > 2.3, and that they had a 73.3% and a 98.3% specificity, respectively.
Tataroglu et al. examined 34 patients (38 nerves, 4 bilateral patients) looking at differences in NCV and SNAP amplitudes in both proximal and distal segments of the nerve. They reported that NCV was significantly different at the proximal segment (p = 0.0001), but not significantly different at the distal segment (p = 0.18). They also noted that SNAP amplitude was significantly lower in both the proximal segment (p = 0.002) and the distal segment (p = 0.003). An important consideration in the work by Tataroglu et al. was the appreciation that SNAP could only be recorded in 68.4% of nerves (26/38). The authors noted that this inability to accurately record SNAP limited its diagnostic potential.
SSEPSSEPs for the diagnosis of MP have been used in comparison to SCS and the reports on which test (SSEP, SCS) is superior are somewhat contradictory. Seror evaluated the effectiveness of SCS versus SSEP in diagnosing MP in 1999 and 2003 [8, 20]. In 1999, Seror concluded that, when using SCS SNAPs to diagnose MP, there is a 90% accuracy, while, when using SSEP, there was only a 13% accuracy with a reported SSEP latency of 29.6 ± 1.6 m/s in asymptomatic limbs and 30.9 ± 1.9 m/s in symptomatic limbs (p > 0.05). He noted that SSEP were recordable in 90% of nerves (26/30) while SNAP was recordable in 56.7% of nerves (17/30). In 2003, Seror looked at using SSEP in 21 patients, using two methods of stimulation, thigh and anterior superior iliac spine (ASIS). He reported that SSEP with ASIS stimulation showed no significant difference in latency of amplitude (p > 0.05) and overall SSEP with ASIS stimulation had a sensitivity of 5% and a specificity of 95%. SSEP with thigh stimulation showed no significant difference in latency but was significantly different in amplitude (p < 0.05), while SSEP with thigh stimulation had a 52% sensitivity and 76% specificity. He noted that SSEP with ASIS stimulation was recordable in 95.2% (20/21) of patients and that SSEP with thigh stimulation was recordable in 52.3% (11/21) patients, overall concluding that SSEP had no diagnostic value for its time. Both Spevak and Prevec and Seror concluded that SCS was the superior electrophysiological study for diagnosing MP.
El-Tantawi [21] studied SNAP and SSEP in 32 patients with known MP. The results showed significant differences between the MP nerves and healthy nerves in all the same metrics as Seror: distal latency, conduction velocity and SNAP amplitude (P < 0.001 for all metrics). When looking at SSEP, El-Tantawi also noted significant differences in conduction and amplitude (p < 0.001 for both metrics), and noted that SNAP abnormality had a 62.3% sensitivity to MP while dermatomal SSEP had a 81.3% sensitivity. Thus, El-Tantawi suggested that, when readable, both SSEP and SCS were equally viable diagnostic tools. However, El-Tantawi also noted that SCS was only obtainable in 71.9% (23/32) of patients, while SSEP was recordable in all patients; this difference in respect to recordability was significant (p < 0.001). Thus, El-Tantawi lent towards SSEP as a preferable diagnostic tool for MP due to its recordability (Table 2).
Table 2 Characteristics of studies using neurophysiology techniques (nerve conduction studies and SSEPs) to diagnose meralgia parestheticaManagementOf the 23 eligible management papers, 4 discussed injection therapy alone [12, 22, 23, 25], 10 discussed surgery [25, 27,28,29,30,31,32,33,34,35], 2 discussed radiofrequency ablation [38, 39], 3 discussed a combination of management options [11, 24, 36] and there was 1 paper for each of botox [39], acupuncture [40], kinesio taping [41] and muscle energy technique [42].
Injection TherapyFour interventional studies were found that looked at steroid injection therapy alone as a management strategy for MP: Tagliafico et al. [12], Klauser et al. [22], Kloosterziel et al. [23] and Kilic et al. [25].
Tagliafico et al. [12] treated 20 patients (7 male, 13 female) with perineural injections of 1 mL of methylprednisolone acetate (40 mg/mL) and 8 mL of mepivacaine, 2%, under direct ultrasound guidance. They found that 16/20 patients reported symptom improvement after one injection and 1 week. The remaining 4 patients had a further injection and all 20 patients reported complete resolution of symptoms at 2 months. Mean visual analogue scale (VAS) score symptom reduction was 8.1 ± 2.1 to 2.1 ± 0.5 (p < 0.001) and VAS quality of life reduction was 6.9 ± 3.2 to 2.3 ± 2.5 (p < 0.002). 5 patients reported sharp thigh pain on needle insertion, all of which were resolved by needle repositioning. No patients reported post-injection side effects.
Klauser et al. [22] performed injections in 20 patients (9 male, 11 female) using a 27G needle with a mixture of 1 ml triamcinolone acetonide (10 mg/ml), and 5 ml of 0.5% bupivacaine. They found that 15/20 reported complete symptom relief and the remaining 5 reported partial symptom relief. Mean VAS score, out of 100, reduced from 82 to 0 in the complete relief group (p < 0.0001) and from 92 to 42 in the partial relief group (p < 0.001). No pain or side effects were reported during injection or post-injection either immediately or at 12-month follow-up. Two patients were noted that required a second session of injections.
Both papers noted the potential necessity of multiple injections to achieve symptom control.
Two RCTs were found, Kloosterziel et al. [23] and Kilic et al. [
留言 (0)