
記住我

From 1990 to 2021, the global burden of migraine significantly increased (Supplementary Material Table S1, Fig. S1). The number of prevalence cases increased from 732.56 million in 1990 to 1.16 billion in 2021, representing an approximate increase of 58.15%. Concurrently, the ASPR increased from 14,027.65 to 14,246.55 per 100,000 population, with an EAPC of 0.06. During the same period, incidence rose from 63.50 million to 90.18 million cases, an increase of 42.06%. Moreover, the DALYs associated with migraine significantly increased from 27.41 million to 43.38 million, an increase of 58.27%. Additionally, the ASDR increased from 526.76 to 532.70 per 100,000 population, with an EAPC of 0.05.
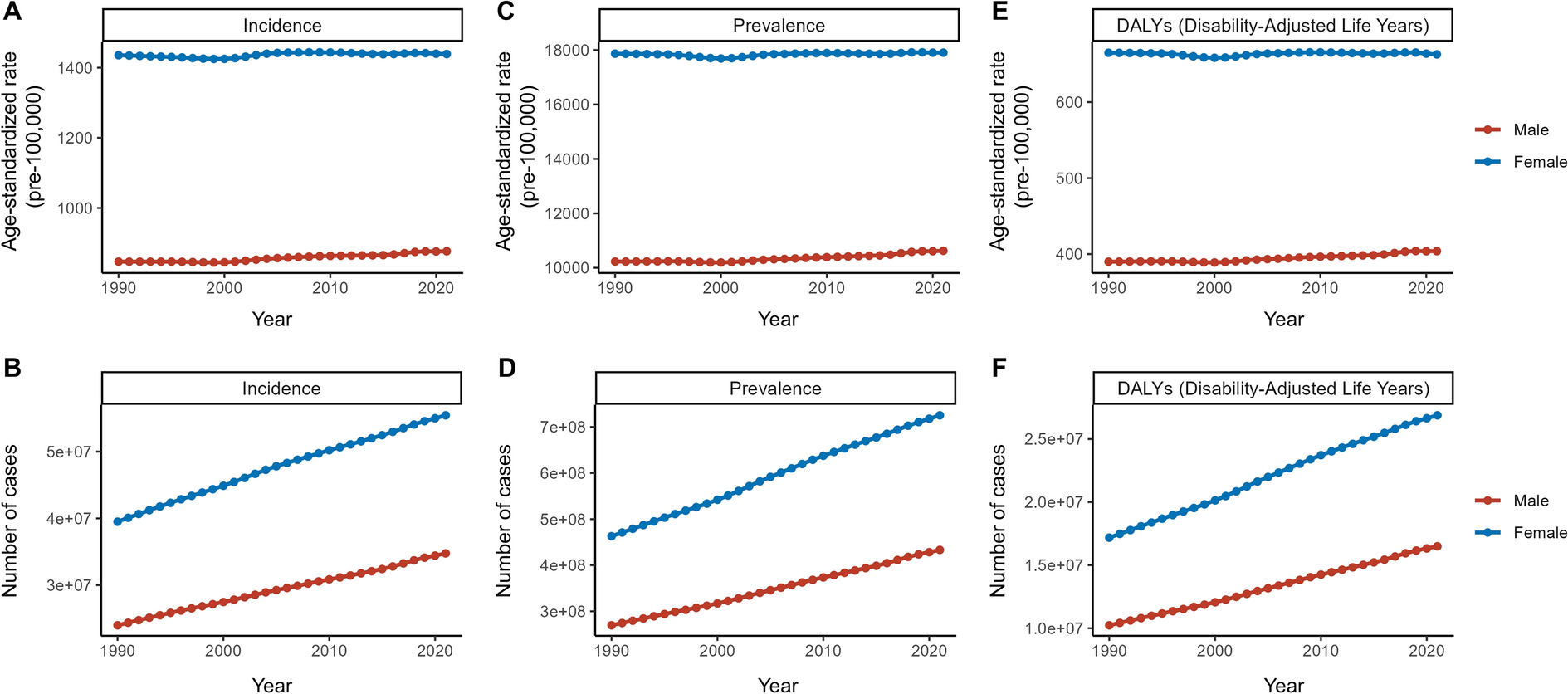
Differences by SexIn 1990, the incidence of migraine in female individuals was approximately 39.50 million, with an ASIR of 1,435.6 per 100,000. By 2021, this figure had increased to 55.43 million cases with an ASIR of 1,438.9 per 100,000 and an EAPC of 0.03. For male individuals, the incidence of migraine in 1990 was 23.99 million, with an ASIR of 846.91 per 100,000. By 2021, this had increased to 34.75 million cases with an ASIR of 876.55 per 100,000 and an EAPC of 0.13, which was fourfold greater than in female individuals (Supplementary Material Table S1).
In 1990, the prevalence of migraine in female individuals was 462.90 million, with an ASPR of 17,864.62 per 100,000. By 2021, this had increased to 725.24 million, with an ASPR of 17,902.6 per 100,000 and an EAPC of 0.02. In 1990, the prevalence of migraine in male individuals was 269.67 million, with an ASPR of 10,229.25 per 100,000. By 2021, this had increased to 433.19 million, with an ASPR of 10,624.2 per 100,000 and an EAPC of 0.13. These data demonstrate that although female individuals have exhibited higher absolute rates of migraine incidence and prevalence in the past, the rate of increase in these parameters have been more rapid in male individuals (Supplementary Material Table S1, Fig. 1, Fig. S2).
Fig. 1
Trends in migraine burden by sex from 1990 to 2021. ASIR (A) and incidence cases (B), ASPR (C) and prevalence cases (D), and ASDR (E) and DALYs cases (F) for migraine between the sexes from 2019 to 2021. ASDR age-standardized DALY rate, ASIR age-standardized incidence rate, ASPR age-standardized prevalence rate, DALYs disability-adjusted life years
Age-Specific TrendsFor both male and female individuals, the ASIR for migraine peaked at 10–14 years old, whereas the ASPR and ASDR increased from the 10–14 years age group to the 40–44 years age group (Supplementary Material Table S2). The ASIR for the 10–14 years age group was 2368.93; the ASIR for the 40–44 years age group was 21,579.93, and the ASDR was 820.79. Prevalence and DALY cases were highest in the 30–34 years age group because this had the greatest population, with 128.09 million and 4.71 million, respectively (Fig. 2).
Fig. 2
Cross-section (2021) of incidence rate, prevalence rate, and DALY rate for migraine across age groups. ASIR (A) and incidence cases (B), ASPR (C) and prevalence cases (D), and ASDR (E) and DALYs cases (F) for migraine. ASDR age-standardized DALY rate, ASPR age-standardized prevalence rate, DALYs disability-adjusted life years
Since the long-term trends in ASR within the 5-year age groups are not pronounced (Supplementary Material Table S2, Fig. S3), we conducted further analysis using broader age groups: “< 20 years,” “20–54 years,” and “> 55 years.” ASIR for adolescents (under 20) was higher than that of the other two groups, with their ASPR and ASDR showing significantly faster EAPC of 0.17 and 0.18, respectively. In contrast, the other two groups exhibited relatively stable trends, with EAPC ranging from −0.03 to 0.05. In 2010, the young to middle-aged group (20–54) had the highest ASPR at 20,380.33, along with the highest ASDR at 763.55 (Supplementary Material Table S2, Fig. 3).
Fig. 3
Trend in globally burden of migraine by age groups (< 20, 20–54, > 55) from 1990 to 2021. Trend in the ASIR (A) and incidence cases (B), ASPR (C) and prevalence cases (D), and ASDR (E) and DALYs cases (F) for migraine from 1990 to 2021. ASDR age-standardized DALY rate, ASIR age-standardized incidence rate, ASPR age-standardized prevalence rate, DALYs disability-adjusted life years
Differences by SDI RegionFrom 1990 to 2021, the burden of migraine varied significantly across different SDI regions (Supplementary Material Table S1, Fig. 4, Fig. S4). The ASIR, ASPR, and ASDR in high SDI areas were highest: 1,222.54, 15,365.14, and 573.62, respectively. The ASIR, ASPR, and ASDR in low SDI areas were lowest: 1,045.99, 12,808.97, and 475.21, respectively. However, the medium SDI and low to medium SDI populations are huge, the number of people who experience migraine in these groups includes more than half of the global population, and the resulting disease burden is considerable.
Fig. 4
Cross-section (2021) of incidence rate, prevalence rate, and DALY rate for migraine across SDI regions. ASIR (A) and incidence cases (B), ASPR (C) and prevalence cases (D), and ASDR (E) and DALYs cases (F) for migraine. ASDR age-standardized DALY rate, ASIR, age-standardized incidence rate, ASPR age-standardized prevalence rate, DALYs disability-adjusted life years, SDI sociodemographic index
In the medium to high SDI region, both ASIR and ASPR increased, with EAPC of 0.15 and 0.10, respectively, whereas the increase in ASDR was only 0.08. The high SDI region exhibited relatively stable trends, with minimal increases in ASIR and ASPR, EAPC of 0.08 and 0.02, and a negligible change in ASDR, EAPC of 0.02. Conversely, the low to medium SDI region showed slight declines in both ASIR and ASPR, with EAPCs of −0.03 and −0.02. In the low SDI region, incidence and prevalence were almost unchanged, whereas ASDR exhibited a slight increase, with an EAPC of 0.03. The medium SDI region showed the most significant increases, with ASIR and ASPR exhibiting EAPCs of 0.16 and 0.19, respectively, highlighting a marked increase in migraine burden (Supplementary Material Table S1, Fig. 4).
Differences by Region and CountryThe global burden of migraine exhibited considerable variation across different regions (Supplementary Material Table S3). Increases were most significant in East Asia and Latin America, with an EAPC of 0.28 for prevalence and 0.26 for DALYs. In Andean Latin America, the EAPCs for prevalence and DALYs were 0.23 and 0.21, respectively; Southern and Tropical Latin America also demonstrated notable upward trends. The most significant decrease in EAPC was observed in Southeast Asia, with a prevalence rate of −0.07, and the EAPC for DALYs was −0.06. However, despite increases in absolute migraine cases in other regions, the incidence and prevalence rate EAPC remained relatively stable here.
In terms of countries (Supplementary Material Table S4, Fig. 5), incidence rate, prevalence, and DALYs increased most in Singapore, with EAPCs of 0.41, 0.48, and 0.4, respectively. Incidence decreased most in South Korea, with an EAPC of −0.18, whereas prevalence and DALYs decreased most in Thailand, with EAPCs of −0.31 and −0.29, respectively. Brazil had the highest ASIR (1510.77) but Belgium had the highest ASPR (21,751.47) and ASDR (800.36). Detailed data are provided in Supplementary Material Table S4.
Fig. 5
National age-standardized incidence, prevalence, and DALY rates for migraine in 2021, with EAPC from 1990 to 2021. ASIR (A), ASPR (B), and ASDR (C). EAPC of ASIR (D), ASPR (E), and ASDR (F) from 1990 to 2021. ASDR age-standardized DALY rate, ASIR age-standardized incidence rate, ASPR age-standardized prevalence rate, DALYs disability-adjusted life years, EAPC estimated annual percentage changes
Correlation AnalysisAs the SDI increased, there was a general trend for increasing migraine ASIR, ASPR, and ASDR (Fig. 6). This upward trend is relatively stable for SDI values of 0.5–0.7 but increases considerably above a value of 0.7, suggesting that countries with high SDI tend to report higher migraine burdens. The ASIR, ASPR, and ASDR of migraine is not significantly related to its EAPC (P > 0.05, Supplementary Material Fig. S5A–5C). Fig. S5D–5E shows that the human development index (HDI) is positively correlated with the EAPC of ASIR and ASPR of migraine (P < 0.01, ρ = 0.20 and P = 0.02, ρ = 0.19), but not significantly correlated with ASDR (P = 0.14, Fig. S5F).
Fig. 6
The correlation between SDI and ASR of migraine in 2021. ASIR (A), ASPR (B), and ASDR (C). ASDR age-standardized DALY rate, ASIR age-standardized incidence rate, ASPR age-standardized prevalence rate, ASR age-standardized rate, SDI sociodemographic index
Frontier AnalysisA comprehensive frontier analysis of different countries and regions of migraine from 1990 to 2021 exhibit marked heterogeneity in the prevention and control. In theory, the burden of migraine should exhibit an downward trend with increasing SDI, and the frontier remained steady after the SDI exceeded 0.25; death rate and DALYs should also followed a similar pattern. The visual representations revealed marked differences among countries. A total of 15 countries (including Brazil, Belgium, Italy, Paraguay, and Norway) had significantly higher prevalence rates and were far from the frontier. Conversely, countries with low SDI (< 0.5), such as Comoros, Burundi, Djibouti, Ethiopia, and Somalia were closer to the frontier, indicating more optimal outcomes relative to their SDI. Countries with high SDI (> 0.85) such as Belgium, Germany, Sweden, San Marino, and Norway exhibited larger deviations from the frontier, indicating a heavier burden. In the DALYs analysis, countries such as Belgium, Italy, and Germany exhibited large deviations from the frontier. Detailed frontier analyses of ASIR, ASPR, and ASDR across countries are presented in Fig. 7 and Supplementary Material Table S5.
Fig. 7
Frontier analysis of migraine in 204 countries and regions in 2021. The gap in ASIR (A, B), ASPR (C, D), and ASDR (E, F) between different countries and the frontier. The frontier represents the ideal level of control. The top 15 countries furthest from the frontier are marked in black; countries with low SDI (< 0.5) and nearest to the frontier are marked in blue; countries with high SDI (> 0.85) and furthest from the frontier are marked in red. Red dots indicate an increase in ASR from 1990 to 2021; blue dots indicate a decrease in ASR from 1990 to 2021. ASDR age-standardized DALY rate, ASIR age-standardized incidence rate, ASPR age-standardized prevalence rate, SDI sociodemographic index
Predictive Analysis for 2050Projections for migraine burden from 2022 to 2050 reveal a notable disparity in growth rates between the sexes, with male individuals expected to experience a more rapid increase than female individuals (Supplementary Material Table S6, Fig. 8). By 2050, the prevalence of male patients is expected to reach 586.96 million, with the number of female patients expected to reach 973.71 million (Fig. 8B). The ASIR for male individuals is expected to increase from 876.55 in 2021 to 907.55 per 100,000 people in 2050, an increase of 3.53%, whereas the ASIR for female individuals is expected to increase only slightly, from 1438.9 to 1445.75 per 100,000 people, an increase of 0.47% (Fig. 8A). Moreover, the growth patterns in ASPR and ASDR are similar: the ASPR for male individuals is expected to rise from 10,624.2 in 2021 to 11,652.14 in 2050 per 100,000 people, an increase of 9.68%, and the ASDR for male individuals is expected to rise from 403.88 in 2021 to 421.77 in 2050 per 100,000 people, an increase of 4.43% (Fig. 8C). The corresponding increases in ASPR and ASDR for female individuals are expected to be much smaller (Fig. 8A, B), with ASPR increasing by 0.36% from 17,902.6 in 2021 to 17,967.77 in 2050 per 100,000 people and ASDR increasing by 0.11% from 662.76 in 2021 to 663.46 in 2050 per 100,000 people (Fig. 8C). Regardless of the ASIR, ASPR, or ASDR, the trend of migraine has significantly increased more among male individuals than among female individuals.
Fig. 8
Trends in observed and predicted global burden of migraine by sex from 2021 to 2050. A The number of incidence cases and its ASIR from 2021 to 2050; B the number of prevalence cases and its ASPR from 1990 to 2050; C the number of DALYs cases and its ASDR from 2021 to 2050. ASDR age-standardized DALY rate, ASIR age-standardized incidence rate, ASPR age-standardized prevalence rate, DALYs disability-adjusted life years
The predictive analysis by age group highlights significant changes in ASIR and ASPR for adolescents (< 20 years) with migraine (Supplementary Material Table S6, Fig. 9). The ASIR is expected to increase from 1395.94 per 100,000 people in 2021 to 1497.09 in 2050 (Fig. 9B), representing a growth of 7.25%. During the same period, the ASPR is projected to rise from 7805.07 to 11,340.41 per 100,000 people (Fig. 9D), an increase of 45.30%. The ASDR across all age groups is expected to remain relatively stable.
Fig. 9
Trends in observed and predicted of global burden of migraine by age groups (< 20, 20–54, > 55) from 2021 to 2050. A The number of incidence cases and its ASIR for age groups from 2021 to 2050; B the number of prevalence cases and its ASPR for age groups from 1990 to 2050; C the number of DALYs cases and its ASDR for age groups from 2021 to 2050. ASDR age-standardized DALY rate, ASIR age-standardized incidence rate, ASPR age-standardized prevalence rate, DALYs disability-adjusted life years
留言 (0)