
記住我
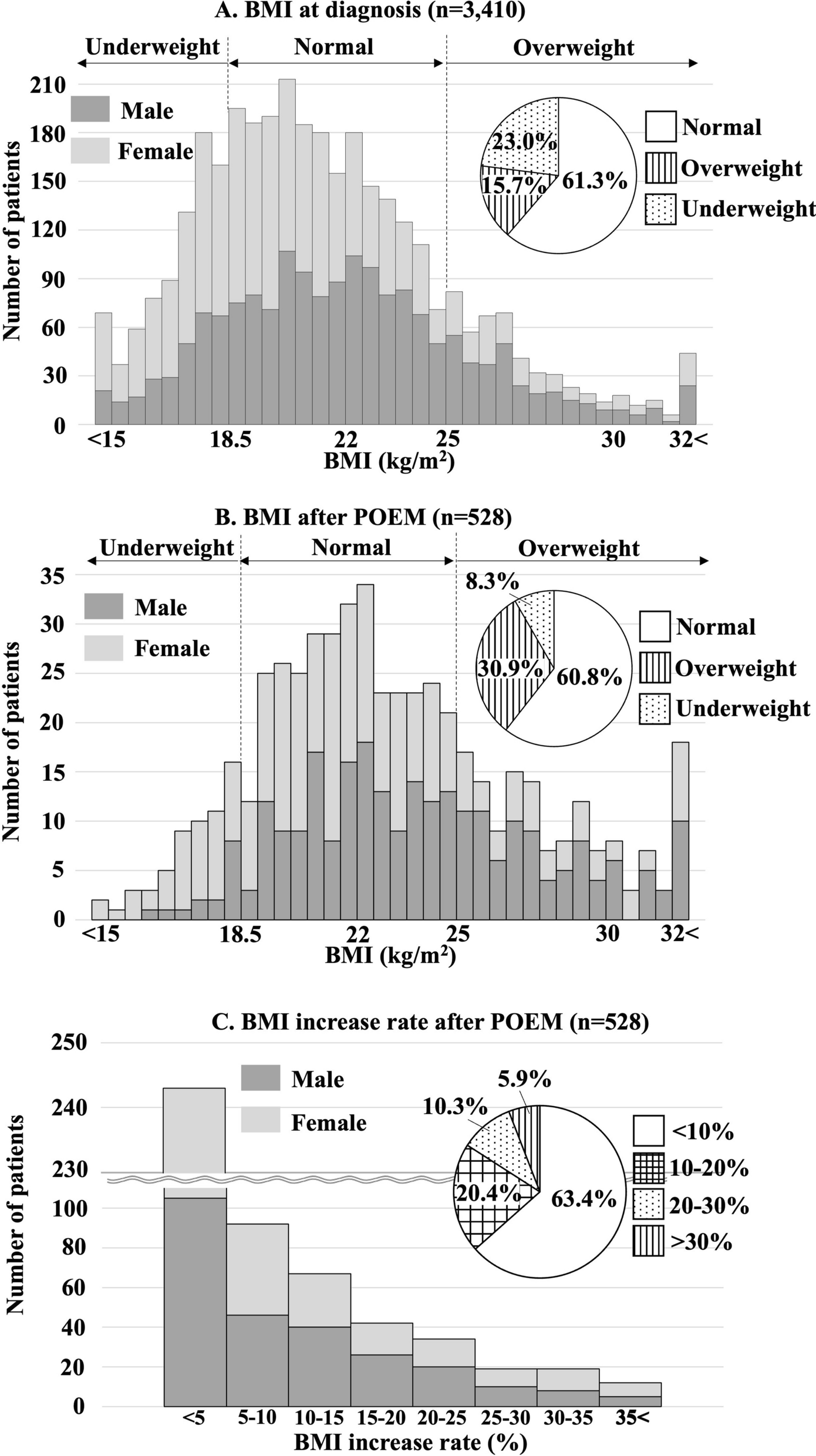


This study included 296 patients with HCC receiving immunotherapy, whose baseline characteristics are detailed in Table 1. In the training set, the median age of patients was 56 years, while in the validation set it was 57 years. Over 88% of individuals in the training group and over 86% of individuals in the validation group were male. The median body mass index (BMI) was 22.49 (20.31, 24.61) kg/m2 and 21.47 (20.33, 24.45) kg/m2 in the training and validation sets, respectively. The patients with hepatitis B in the training set was 90.40% compared to 88.98% in the validation set. In the training set, there were 133 patients classified as Child–Pugh class A (75.14%) and 44 as class B (24.86%). The validation set included 91 patients classified as A (76.47%), 27 as B (22.69%), and 1 as C (0.84%). In the training and validation groups, 98.87% and 99.16% of patients had an ECOG PS score of 0–1, respectively. 52 (29.38%) of patients had postoperative recurrence and 90 (50.85%) had prior transcatheter arterial chemoembolization (TACE) treatment in the training set, which was not statistically different from the validation set. In the training set, 115 patients (64.97%) received first-line immunotherapy and 62 patients (35.03%) received second or later line immunotherapy; while in the validation set, 71 patients (59.66%) received first-line immunotherapy and 48 patients (40.34%) received second or later line immunotherapy. 41.24% of patients in the training set were treated with a combination of targeted therapy compared to 37.82% in the validation set. In addition, macrovascular invasion was observed in 83 patients (46.89%) in the training set and 55 patients (46.22%) in the validation set. In the training set, extrahepatic spread was present in 81 patients (45.76%), while it was present in 49 patients (41.53%) of the validation set. The BCLC stages for the training and validation sets were as follows: n = 9 (5.08%) vs. n = 6 (5.04%) for stage 0, n = 10 (5.65%) vs. n = 9 (7.56%) for stage A, n = 26 (14.69%) vs. n = 27 (22.69%) for stage B, and n = 132 (74.58%) vs. n = 77 (64.71%) for stage C, respectively. The baseline characteristics did not show statistically significant variance between patients in the training and validating sets (P > 0.05).
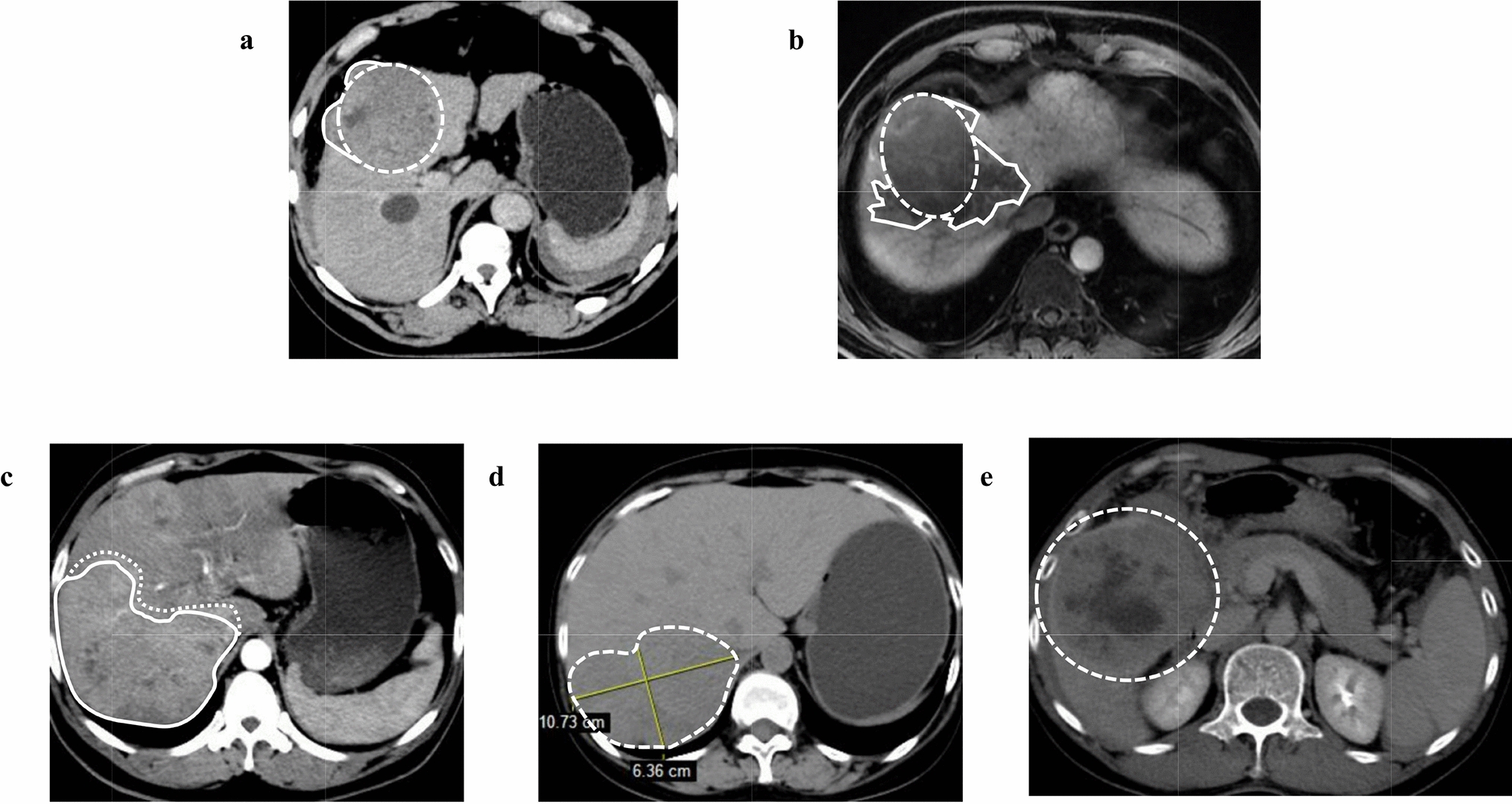
Table 1 Patient characteristics of the training and validation cohortThe AFP value before immunotherapy was used to create the ROC curve, which determined the optimal cutoff value of 386.43 ng/ml for AFP (Fig. S2). After rounding, the individuals were divided into categories of high and low AFP levels using a cut-off value of 400 ng/ml. 72 patients (40.68%) exhibited AFP levels ≥ 400 ng/ml, and 105 (59.32%) patients exhibited AFP levels < 400 ng/ml. The initial tumor shape was irregular in 98 patients (55.37%) and regular in 79 patients (44.63%).
Univariate and multivariate Cox regression analyses of OS and PFS in the training setIn the multivariate Cox regression analysis of OS, baseline AFP ≥ 400 ng/ml and initial tumor shape irregularity were found to be significant independent prognostic factors for OS after adjusting for potential confounders (AFP ≥ 400 ng/ml, HR 1.73, 95% CI 1.01–2.96, P = 0.046; Initial tumor shape irregularity, HR 1.94, 95% CI 1.03–3.65, P = 0.041; Table 2). The irregular shape of the tumor is a significant predictor of progression-free survival based on the multivariate analysis (HR 2.15, 95% CI 1.40–3.29, P < 0.001).
Table 2 Results of univariate and multivariate Cox regression analysis of OS and PFS in the training cohortAFP ≥ 400 ng/ml and the initial tumor shape irregularity were both identified as significant prognostic factors for OS. In addition, the hazard ratios (HRs) for both factors were similar in multivariate analyses. Therefore, we devised a simple score for forecasting prognosis based on these two variables, named ATSI (AFP and Tumor Shape Irregularity). One point was assigned to each AFP ≥ 400 ng/ml or irregular initial tumor shape, thus dividing patients into three groups: ATSI score 0 points (AFP < 400 ng/ml and initial tumor shape regularity); ATSI score 1 point (AFP ≥ 400 ng/ml or initial tumor shape irregularity); ATSI score 2 points (AFP ≥ 400 ng/ml and initial tumor shape irregularity). Furthermore, the patients with higher AFP levels exhibited notably inferior median OS and PFS outcomes compared to those with lower AFP levels [median OS, 17.60 (95% CI 13.30–26.43) vs. 28.20 (95% CI 21.93–NA) months, P = 0.005; median PFS, 6.17 (95% CI 5.03–11.60) vs. 9.23 (95% CI 8.37–10.93) months, P = 0.041]. The median OS and PFS of patients with regular tumor shape were 38.93 months (95% CI 26.43–NA) and 10.17 (95% CI 9.23–13.40) months, respectively, which were significantly superior to those with irregular shapes [median OS, 18.13 months (95% CI 15.17–25.80), P = 0.008; median PFS, 6.43 months (95% CI 5.33–8.13), P < 0.001]. OS and PFS survival curves for AFP and initial tumor shape irregularity are shown in Fig. 2a–d.
Fig. 2
OS and PFS survival curves for AFP and irregular tumor shape. a Overall survival and b progression-free survival for baseline AFP level. c Overall survival and d progression-free survival for the irregular tumor shape
Objective efficacy and survival analysis in the training setThe complete follow-up imaging was available for 166 (93.79%) patients in the training set. 77 (43.50%) patients reached the endpoint of death. 110 (62.15%) patients with confirmed progressive disease at final analysis. In the training set, the median OS was 22.6 months (95% CI 18.13–NA), while the median PFS was 9.07 months (95% CI 7.87–10.10, Table 3). At the time of analysis, the best radiological response was as follows: CR, n = 13 (7.83%); PR, n = 21 (12.65%); SD, n = 91 (54.82%); and PD, n = 41 (24.70%) (Table 3). As a result, 125 patients achieved disease control with the disease control rate (DCR) of 75.30% and 41 patients achieved objective remission with the objective response rate (ORR) of 24.70%.
Table 3 Objective efficacy and survival analysis according to ATSI score in the training setEfficacy and survival prediction according to ATSI score in the training setThe training set cohort was stratified according to ATSI scores, resulting in 53 (29.94%) patients with 0 points, 77 (43.50%) patients with 1 point, and 47 (26.56%) patients with 2 points. The 1-year OS rate was 71.70%, 54.55%, and 53.19% in 0 points, 1 point, and 2 points (P = 0.090, Fig. 3a), respectively. The median OS was not reached in patients with 0 points (95% CI 28.20–NA), and the median OS was 25.80 (95% CI 14.17–NA) months in patients with 1 point, 17.03 (95% CI 11.73–23.83) months in patients with 2 points (P = 0.001, Table 3). In the training set, the median PFS was 10.83 (95% CI 9.27–14.33) months for ATSI score 0 points, 8.03 (95% CI 6.77–10.57) months for ATSI score 1 point, and 5.03 (95% CI 3.83–9.67) months for ATSI score 2 points (P < 0.001, Fig. 3b).
Fig. 3
Kaplan–Meier curves for the training and validation sets according to ATSI score. a Overall survival and b progression-free survival for the training set according to ATSI score. c Overall survival and d progression-free survival for the validation set according to ATSI score
The best radiological response for each group after stratification according to ATSI score was as follows: CR was n = 3/49 (6.12%) vs. n = 8/73 (10.96%) vs. n = 2/44 (4.55%), and PR was n = 5/49 (10.20%) vs. n = 12/73 (16.44%) vs. n = 4/44 (9.09%) for ATSI-0 points vs. ATSI-1 point vs. ATSI-2 points, respectively; SD was n = 35/49 (71.43%) vs. n = 39/73 (53.42%) vs. n = 17/44 (38.64%), and PD was n = 6/49 (12.24%) vs. n = 14/73 (19.18%) vs. n = 21/44 (47.73%) for ATSI-0 points vs. ATSI-1 point vs. ATSI-2 points, respectively. DCR was 87.76%, 80.82%, and 52.27% in the 0 points, 1 point, and 2 points groups, respectively (P < 0.001, Table 3).
Efficacy and survival prediction according to ATSI score in the validation setThe validation set included 119 HCC patients who received immunotherapy, of which 116 (97.48%) patients had complete imaging data. The best radiological response results in the validation cohort at the final analysis showed 9 (7.76%) patients in CR, 18 (15.52%) patients in PR, 59 (50.86%) patients in SD and 30 (25.86%) patients in PD (Table 4). ORR was 23.28% in the validation set, while DCR was 74.14%. The progressive disease was confirmed in 74 (62.18%) patients, with the median PFS of 8.30 months (95% CI 6.73–11.87, Table 4). 49 (41.18%) patients died at the final analysis, with the median OS of 28.10 months (95% CI 19.83–NA, Table 4).
Table 4 Objective efficacy and survival analysis according to ATSI score in the validation setThe results of the ATSI score were as follows: ATSI-0 points, n = 37 (31.09%); ATSI-1 point, n = 48 (40.34%); and ATSI-2 points, n = 34 (28.57%). Kaplan–Meier survival curves according to ATSI score showed significant differences in PFS and OS among the three groups of patients (Fig. 3c, d). The median OS for patients with 0 points was 37.43 (95% CI 28.10–NA) months, which was significantly better than patients with 1 point at 24.27 (95% CI 18.23–NA) months and patients with 2 points at 14.03 (95% CI 12.37–NA) months (P = 0.028). The median PFS was 13.93 (95% CI 10.73–NA) months for 0 points, 8.30 (95% CI 6.73–16.33) months for 1 point and 4.90 (95% CI 3.00–9.03) months for 2 points (Table 4).
In the validation set, CR or PR was achieved in 10 (27.78%) patients with ATSI-0 points, in 11 (23.91%) patients with ATSI-1 point, and 6 (17.65%) patients with ATSI-2 points. Among the patients with stable diseases, there were 21 (58.33%) with 0 points, 25 (54.35%) with 1 point, and 13 (38.24%) with 2 points. 5 (13.89%) patients with 0 points, 10 (21.74%) with 1 point, and 15 (44.12%) with 2 points achieved progressive disease. The DCR was 86.11% for 0 points, 78.26% for 1 point, and 55.88% for 2 points, respectively (P = 0.011, Table 4).
Objective response analysis after adjustment in the training and validation setsConsidering that some patients had incomplete follow-up imaging (6.21% in the training set; 2.52% in the validation set), we analyzed them according to the worst-case scenario and assigned all patients with missing follow-up imaging data to the PD group and the differences in DCR between the groups stratified by the ATSI score were still statistically significant (Table S1). Based on this, the ATSI score was effective in predicting tumor response in HCC patients receiving immunotherapy.
In the multiple comparisons between each group, we found that the differences in best radiological response and DCR were not statistically significant in those ATSI-0 points versus ATSI-1 point in both the training and validation sets (P > 0.05). However, the radiological response and DCR were significantly superior in both patients with ATSI-0 points and ATSI-1 point than ATSI-2 points in both the training and validation sets (P < 0.05).
Efficacy and survival prediction according to ATSI score in the overall populationAdditionally, we have tested the effects of AFP and tumor shape irregularity in the overall population. The results showed that patients with AFP ≥ 400 ng/ml had inferior OS and PFS than those with AFP < 400 ng/ml (P < 0.05, Fig. S3ab) and patients with irregularly shaped tumors also had significantly worse OS and PFS than those with regular shapes (P < 0.001, Fig. S3cd). Subsequently, we tested the efficacy of the ATSI score in the overall population, both the OS and PFS in patients with 0 points were the longest, followed by patients with 1 point, and patients with 2 points had the worst OS and PFS (P < 0.001, Fig. S4). In addition, we analyzed the impact of prior TACE therapy and first-line or second/later-line immunotherapy on patients’ survival. The results showed that the predictive performance of the ATSI score is well represented in both first-line and second/later-line immunotherapy populations (Fig. S5). Similarly, the ATSI score showed a good predictive performance in the population with or without prior TACE treatment (Fig. S6). Furthermore, we found that the ATSI score also showed a favorable predictive effect in both early/intermediate-stage and advanced-stage HCC patients (P < 0.05, Fig. S7).
Of the 184 patients with tumor progression, 111 patients were treated with subsequent immunotherapy after tumor progression, whereas targeted therapy was applied to 65 patients, and 56 patients were treated with targeted therapy in combination with immunotherapy. The survival analysis shows that patients who received either immunotherapy alone or targeted therapy combined with immunotherapy had better OS than those who did not receive subsequent therapy (median OS, 37.43 (95% CI 18.13–NA) vs. 28.10 (95% CI 19.80–NA) vs. 14.97 (95% CI 10.87–26.43) months, P = 0.002, Fig. S8). However, there was no statistically significant difference in the prognosis between patients who received immunotherapy alone and the patients who received targeted therapy combined with immunotherapy after progression (P > 0.05, Fig. S8).
Albumin-bilirubin (ALBI) grade has been proposed and validated to predict survival benefits for HCC patients receiving immunotherapy, we compared the area under the curve (AUC) and net reclassification improvements (NRI) in predictive performance between ATSI score and ALBI grade (Table S2). The results showed that the ATSI score had higher AUC values compared to the ALBI grade in terms of discriminating survival outcomes, suggesting that the ATSI score has a better discriminatory ability in predicting OS of HCC patients receiving immunotherapy (AUC: 0.627 vs. 0.546, P = 0.039, Fig. S9). In addition, although not statistically significant, continuous NRI analysis showed improved performance of ATSI score compared to ALBI grade, with a 19.8% increase in the percentage of correct predictions [continuous NRI (95% CI): 0.198 (− 0.031 to 0.294), P = 0.096]. We believe that this may be due to the relatively small sample size of our study and the specific characteristics of the patient population.
留言 (0)