In this observational study, we examined the occurrence of CIN following the HSG procedure in women with infertility. Our findings indicate that contrast medium (CM) may adversely affect kidney function after HSG procedure. We also identified that low level of baseline SCr is an independent risk factor for the development of CIN in patients undergoing the HSG procedure. To the best of our knowledge, this is the first study to specifically evaluate the development of CIN in HSG procedures.
While the precise molecular and cellular mechanisms behind CIN actively under investigation, it is thought that arterial vasoconstriction leading to renal medullary hypoxia, along with the direct toxic effects of CM on renal tubular cells, play key roles in the development of CIN [6, 17]. These mechanisms are thought to involve the production of reactive oxygen species (ROS), which can cause mitochondrial dysfunction, cellular apoptosis or necrosis, and interstitial inflammation. Elevated ROS levels or diminished antioxidant enzyme activity contribute to increased oxidative stress and subsequent impairment of renal function [18]. Other contributing mechanisms include reduced vasodilation from decreased prostaglandin and nitric oxide levels, impaired endothelial function, elevated renal adenosine concentration, and an increase in oxygen free radicals due to hyperosmotic load. Additionally, contrast-induced diuresis can lead to increased intratubular pressure, heightened urinary viscosity, and obstruction of the tubules [19].
It is widely recognized that chronic kidney disease (CKD), diabetes mellitus (DM) with compromised renal function, congestive heart failure, volume depletion, advanced age, hypertension, and hyperuricemia are significant risk factors for developing CIN following the use of contrast media (CM). Previous studies have shown that the prevalence of CIN can be as high as 50% in patients with impaired renal function and/or one or more of these risk factors [20].
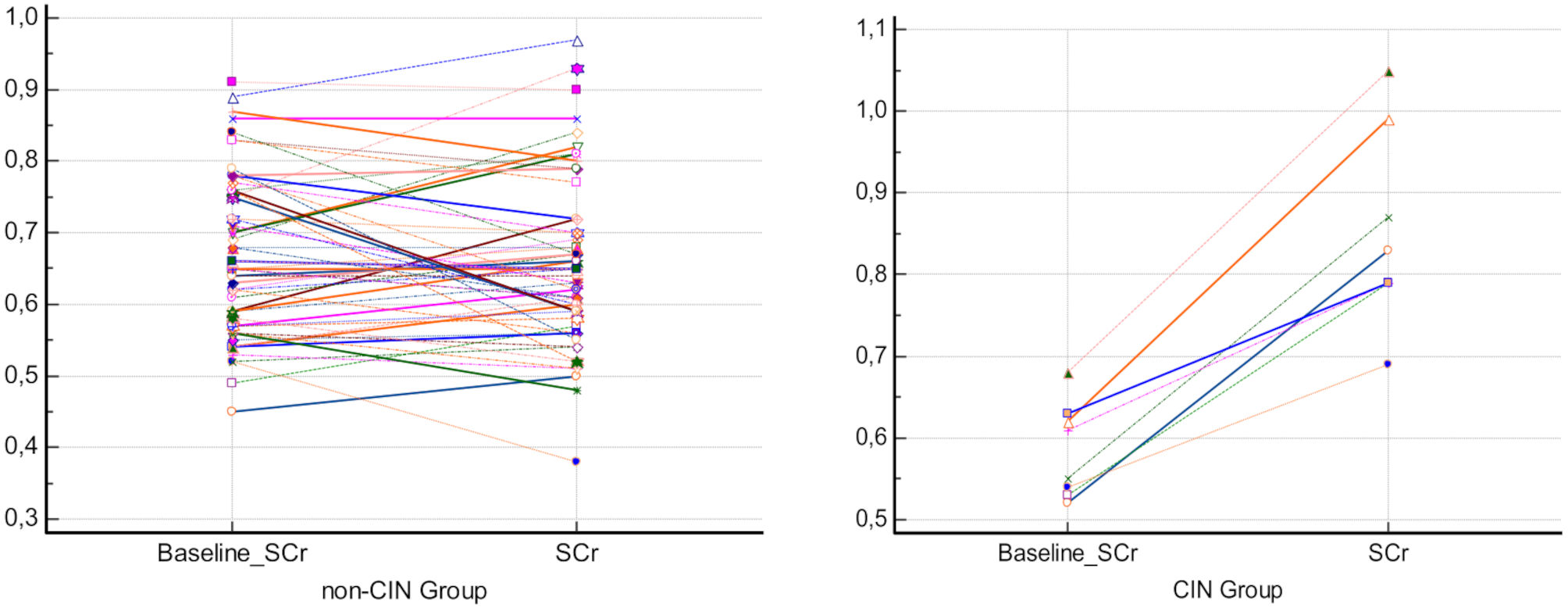
On the other hand, recent studies have indicated that CIN can also occur in patients with normal kidney function who do not present with any of the commonly recognized risk factors [21]. In low-risk groups, the reported prevalence of CIN ranges from 1 to 10% [20, 22, 23]. Consistent with previous studies, we observed a CIN incidence of 12.3% following HSG in female patients with normal renal function. We also noted that one patient (1.2%) experienced severe nephropathy after the HSG procedure. However, all CIN cases were transient and asymptomatic, with renal function returning to normal within one week. This suggests that patients who develop CIN after HSG are underdiagnosed and overlooked.
According to the literature, the development of CIN is affected by various factors, such as female gender, use of iodine-containing antiseptic solutions, and nephrotoxic drugs such as nonsteroidal anti-inflammatory drugs (NSAIDs) used for pain control after hysterosalpingography (HSG) [17, 24,25,26]. Additionally, previous reports have shown that volume expanders, sodium bicarbonate, N-acetylcysteine (NAC), ascorbic acid, statins, and phosphodiesterase type 5 inhibitors help prevent CIN [17, 25, 26]. In this study, both the presence of predisposing risk factors and the lack of preventive measures may have contributed to the development of CIN in our study population. Therefore, we strongly recommended that future studies are needed in this topic.
In the present study, an iodinated, low-osmolar, water-soluble radiocontrast agent was used for HSG, with a typical volume between 5 and 20 ml. In the literature, many studies concluded the type of contrast agent, the volume used, and the route of administration affect the development of CIN. Moreover, some recent studies have suggested that CIN can occur even with very low doses of CM [2]. Additionally, it is known that iodine is a crucial element for life, iodine-containing substances, including antiseptics, medications, topical agents, and contrast agents, may potentially cause nephrotoxicity [27, 28]. We also observed that there was no association between the volume of CM used and the development of CIN in our study population.
The literature identifies a range of modifiable and non-modifiable risk factors for CIN. However, effective strategies for preventing or mitigating CIN remain limited and are often specific to particular procedures or patient populations [29, 30]. In our study, we investigated risk factors associated with the development of CIN and we found that age, intravasation of CM, and lower level of baseline SCr were potential risk factors, particularly in patients with open tubal passages during the HSG procedure. We also identified lower level of baseline SCr as an independent risk factor for CIN development in patients who underwent the HSG procedure.
Our present findings are noteworthy, particularly given that the study population consisted of healthy female patients. A closer analysis of the data reveals that the patient who developed contrast-induced nephropathy (CIN) exhibited a creatinine increase from 0.59 to 0.85. While this increase surpasses the 25% threshold typically required to diagnose CIN, the actual ‘elevated’ creatinine levels still fall within the normal range. Therefore, the statistically significant results of this study can be considered to have no clinical significance. However, based on our current results, it is clear that future long-term studies are needed to examine the potential effects of CIN after HSG on pregnancy and fetal health in this patient population.
Limitations.
It was not possible to create a control group of HSG patients who did not receive contrast material. Therefore, we limited the study to comparing creatinine values before and after HSG. The absence of a non-contrast control group prevents us from drawing definitive conclusions from our data, which is perhaps the biggest limitation of our study.
Other limitations of this study included the small number of participants and the reliance on peripheral blood samples to calculate SCr and eGFR. Additionally, the study lacked other clinical and laboratory parameters, such as genetic factors, complete blood counts, and sodium, albumin, and cholesterol levels, which could influence the development of CIN. These limitations were due to the unavailability of these records.



留言 (0)