
記住我


This study retrospectively analysed all oocyte donation cycles performed between July 2018 and July 2022 in the Department of Reproductive Medicine at the University Hospital of Lille, France.
DonorsAll the donors were younger than 38 years and were recruited by the same referring physician. Donors were systematically evaluated for contraindications such as hereditary conditions or contraindications to controlled ovarian stimulation. Their ovarian reserve was assessed by a serum anti-Müllerian hormone (AMH) assay (Access Anti-Müllerian Hormone [AMH] Assay; Beckman Coulter, Inc.) [8] and an antral follicle count (AFC) [6] using real-time two-dimensional ultrasound (Voluson™ E8 Expert; GE Healthcare) performed during the same consultation.
The assessment was completed by karyotype, psychological evaluation, and human immunodeficiency virus (HIV1–2), hepatitis B virus (HBV), hepatitis C virus (HCV), syphilis, chlamydia and cytomegalovirus (CMV) serology [7].
Women with any hereditary disease, an abnormal karyotype, a body mass index (BMI) > 34 kg/m2, an AMH concentration < 5 pmol/l, an AFC < 8 or abnormal serology were excluded [7].
Phenotypic characteristics (color of skin, eyes and hair, geographic origin, weight and height) and blood group were used to match donors and recipients. A donor was allocated to one or two recipients according to her ovarian reserve and the number of oocytes at the time of oocyte retrieval [7].
RecipientsCouples seeking oocyte donation were seen at a specialized consultation conducted by a single practitioner at the center. Women with premature ovarian failure (idiopathic, iatrogenic, autoimmune or genetic), at risk of maternal genetic disease or couples in intraconjugal ART failure were eligible to receive oocyte donation. In addition, they had to be younger than 40 years at registration, as the average waiting time was estimated to be 2 years. Couples with very severe sperm impairment were mostly referred for embryo donation and were subsequently excluded from oocyte donation. Women with contraindications to oral estrogens were excluded. An interview with a psychologist, serology (HIV 1–2, HCV, HBV, syphilis, CMV and chlamydia), and early recognition of parenthood were required at registration [7].
TreatmentsOne cycle of controlled ovarian stimulation was performed per donor. An antagonist protocol was used, and the gonadotrophin starting dose was individually adjusted according to the AFC, AMH concentration, age and BMI and subsequently adjusted during stimulation according to ultrasound findings and estradiol levels [7].
A bolus of gonadotrophin-releasing hormone (GnRH) agonist (0.2 mg of triptoreline, Decapeptyl®) was administered as soon as at least two dominant follicles with a mean diameter > 18 mm was obtained. Oocyte retrieval was performed by transvaginal ultrasound-guided needle aspiration 36 h after triptoreline injection [7].
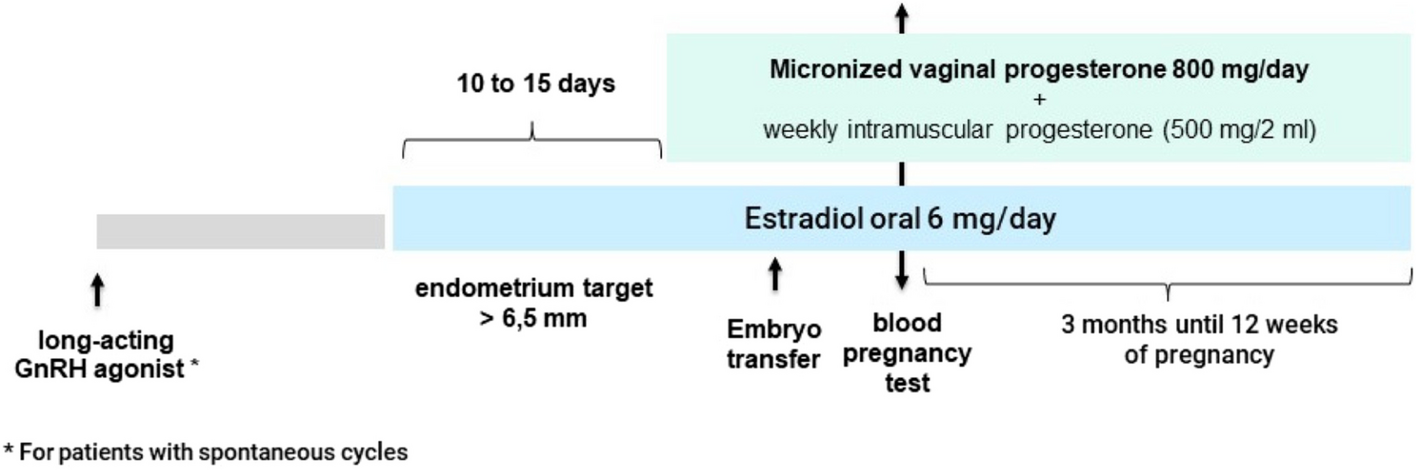
Synchronously with donor stimulation, the recipients received endometrial preparation by hormone replacement treatment with the use of long-acting GnRH agonist (3 mg, triptoreline, Decapeptyl®) if they still had spontaneous cycles. The endometrial preparation used oral micronized oestradiol 6 mg/day (Provames®, oestradiol 2 mg/tablet), and endometrial thickness was checked on day 12 of treatment. When the endometrial thickness was > 6.5 mm, treatment with vaginal micronized progesterone 400 mg twice a day (Progestan®, progesterone 200 mg/caps) or oral dydrogesterone 20 mg twice a day (Duphaston®, dydrogesterone 10 mg/tablet), both associated with weekly intramuscular progesterone (Progesterone Retard®, hydroxyprogesterone caproate 500 mg/2 ml; Bayer Healthcare, France), was initiated on the evening of donor oocyte retrieval.
Sperm microinjection via the ICSI technique with the partner's frozen spermatozoa was performed on each M2 oocyte. Normal diploid fertilization was evaluated 16–18 h after the injection by observing two pronuclei and the second polar body (PB) expelled in the perivitelline space (PVS). Early cleavage was observed 27 h after injection. Embryo quality was estimated at 44–46 h (or 68 h) after injection. Embryo quality classification in our IVF laboratory is based on the number and size of blastomeres, the degree of fragmentation, and the presence or absence of multinucleated blastomeres according to the Istanbul Consensus Conference [1]. On day 2, an embryo was considered to be of good quality if it had 4 blastomeres of equal size, no multinucleation and less than 10% fragmentation. If embryo transfer occurred on day 3 after injection, a good-quality embryo was required to have 8 cells of equal size without multinucleation and with less than 10% fragmentation. Only supernumerary embryos of good quality were frozen for subsequent embryo transfers.
The transfer of cleaved-stage embryo(s) to recipients was performed at D2 or D3 postoocyte retrieval. For frozen embryo transfers, intramuscular supplementation was initiated at the same time as vaginal progesterone or dydrogesterone.
A blood test for hCG assessment was performed 14 days after embryo transfer. Pregnancy was subsequently confirmed via transvaginal ultrasonography at 5–6 weeks of gestation via visualization of the gestational sac.
Clinical pregnancy was defined by an hCG concentration > 100 IU/l 14 days after embryo transfer, with at least one gestational sac visualized by early ultrasound at 6 weeks of pregnancy. Ongoing pregnancy was defined by the ultrasound visualization of at least one gestational sac with an embryo with cardiac activity after 12 weeks of pregnancy. The miscarriage rate was defined as the rate of clinical pregnancy resulting in pregnancy loss by 12 weeks. The live birth rate was defined as the number of deliveries that resulted in a live-born neonate relative to the total number of transfers. The primary endpoint was the clinical pregnancy rate. The secondary endpoints were ongoing pregnancy, live birth and miscarriage rates [7].
From July 2018 to April 2021 (Fig. 1), progesterone was administered to all the recipients by the micronized vaginal progesterone 800 mg per day (Progestan®, progesterone 200 mg/caps: 400 mg twice a day) combined with weekly intramuscular progesterone (Progesterone Retard®, hydroxyprogesterone caproate 500 mg/2 ml; Bayer Healthcare, France).
Fig. 1
Treatment of recipients from July 2018 to April 2021
From April 2021 until July 2022 (Fig. 2), all the recipients received 40 mg of oral dydrogesterone per day (Duphaston®, dydrogesterone 10 mg/tablet: 20 mg twice a day) with weekly intramuscular progesterone.
Fig. 2
Treatment of recipients from April 2021 to July 2022
These various treatments (estradiol, vaginal progesterone or dydrogesterone with intramuscular progesterone) continued until the twelfth week of pregnancy, unless they stopped earlier after a diagnosis of miscarriage.
There were no changes in either the selection of donors or recipients or in any of the laboratory techniques from July 2018 through the end of the study.
Statistical analysisQualitative variables are described in terms of frequencies and percentages. Quantitative variables are described as mean and standard deviation or median (interquartile range) in the case of a non-Gaussian distribution. The normality of the distributions was checked graphically and using the Shapiro‒Wilk test. The initial characteristics of the donors, recipients, their partners, and laboratory parameters were compared between the 2 treatment groups using the chi-square test for qualitative variables and Student’s t test (or the Mann‒Whitney U test in the case of non-Gaussian distribution) for quantitative variables. For further analysis, parameters with missing values were treated by simple imputation. Missing data were imputed under the "missing at random" assumption using the chained equation method with m = 1 imputation. Quantitative variables were imputed by the “predictive mean matching method”, and qualitative variables were imputed by logistic regression models (binomial, ordinal or multinomial). Outcomes were compared between the 2 treatment groups using a logistic regression model adjusted for the confounding factors found (at the 5% threshold). The clinical pregnancy rate was compared between embryo quality grades and between fresh and frozen embryos using the chi-square test. The level of significance was set at 5%. All the statistical analyses were performed using SAS software (SAS Institute version 9.4).
留言 (0)