From the measured lipid parameters, LDL and HDL were significantly different in GDM vs. non-GDM patients even after adjustment for confounders. The LDL/HDL and TC/HDL ratios were most significantly associated with the incidence of GDM in women undergoing IVF/ICSI.
119 (15.5%) of the 767 patients were diagnosed with GDM. This corresponds to the results of a large-scale meta-analysis, which estimated China’s overall GDM rate to be at 14.8% [23]. However, there are significant regional differences: several similar studies with pregnant women in different cities of China found the prevalence of GDM to be at 15.2% [24] and 19.7% in Beijing [25], and 10.5% in Shanghai [26]. Concerning lipid parameters, the prevalence of dyslipidemia amongst adults in China has been estimated to be 34.0%, though it is significantly higher in men and older people [1]. In this cross-sectional analysis, the average age of the participants was 50.24 years, and the rates of dyslipidemia were significantly higher in men (41.9%) than in women (32.5%). In our cohort of women undergoing IVF/ICSI, 30.4% of the study participants had at least one lipid parameter outside the recommended values of the AACE 2017 [21] and Chinese guidelines from 2016 [22], which is comparable to observed dyslipidemia rates in China.
Recorded factors that were significantly associated with GDM were age, BMI, fasting glucose, LH, and E2 (all p < 0.05). Age and BMI are known from the literature as risk factors for GDM [8], as well as hyperglycemia before pregnancy, which is represented by the pre-pregnancy fasting glucose measurement. One study suggested that the FSH/LH ratio could be an early predictor of GDM for women undergoing IVF [27]. A possible explanation could be the relationship between LH and estrogen, whereby the latter is known to be a protective factor against diabetes and modify insulin resistance [28]. Low levels of SHBG (sex hormone binding globulin), which are also closely interrelated with LH levels, are also associated with increased insulin resistance and therefore with the occurrence of GDM [29]. However, the exact mechanisms remain to be further explored.
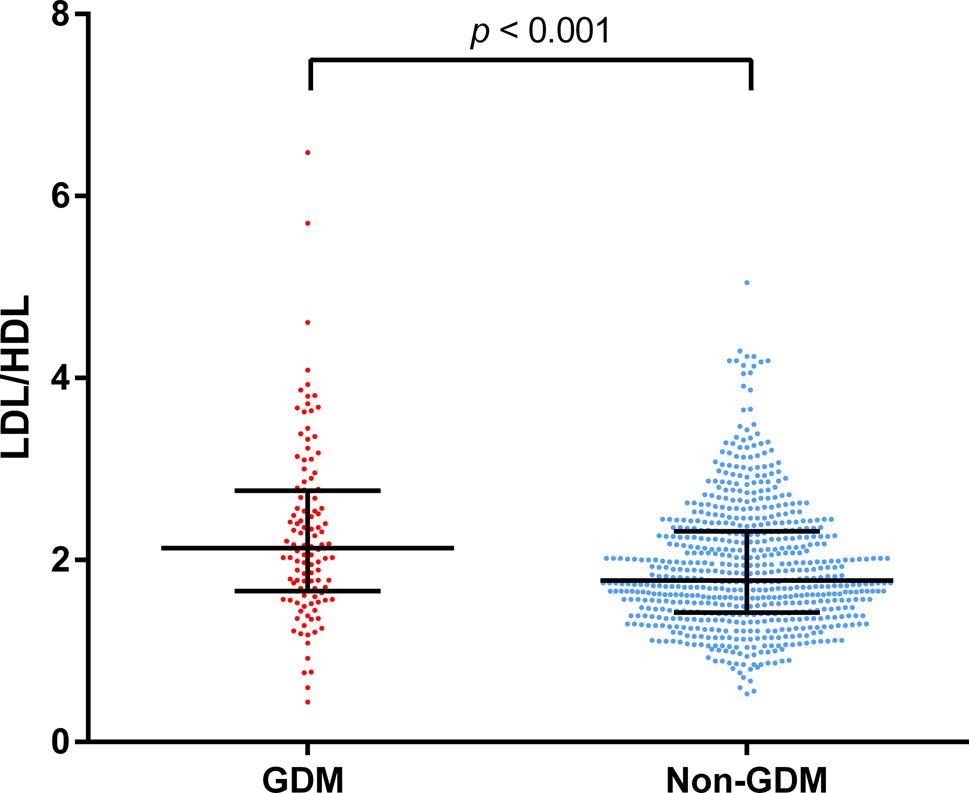
From the initial univariate analysis, three of the four measured lipid parameters, LDL, HDL, and TG, were significantly different in GDM versus non-GDM patients. Of these, HDL showed the strongest association (p < 0.001), whilst TC was not significantly different (p = 0.059). After adjusting for confounding factors, TG also did not show a significant association with GDM (in both Models A and B).
The lipid ratios LDL/HDL and TC/HDL showed strong associations with GDM incidence, even after adjustment for confounders. Looking at binary LDL/HDL for example, it showed a significant odds ratio (OR 1.957 [95%CI 1.258, 3.044], even higher than for BMI with GDM (Supplementary Tables 3a-d)). Our findings suggest that analyzing lipid ratios, along with other known risk factors such as age, baseline fasting glucose, and LH, could be a cost-efficient method to identify women undergoing IVF/ICSI who have a high risk for developing GDM.
Previous studies that also measured the same four lipid parameters as in our study, but in a normally conceived pregnancy, have found that TG and HDL were significantly associated with GDM, but not TC and LDL [2, 30]. Another study in China by Shen et al. [26] found that whilst TG was associated with GDM throughout pregnancy, TC and LDL were only higher in the first trimester in women who developed GDM. This indicates how lipid parameters also significantly change throughout the course of pregnancy. Even though our analysis showed differing results, whereby TG was only significantly associated with GDM in univariate analysis but not after adjustment for confounders, we also found that there was a strong, inverse association with HDL, as well as a positive association with LDL. In addition, many studies did not assess lipid ratios, which, in our study, had the strongest statistical association with GDM. For further studies, it would be meaningful to include calculated lipid ratios, as they may be a better indicator of lipid status [11].
The subgroup analysis in our cohort confirmed that older women, women with a higher BMI, higher pre-pregnancy fasting plasma glucose, blood pressure, as well as low LH showed a higher prevalence of GDM. As seen in Fig. 3, the LDL/HDL ratio also had a significant effect on GDM risk in women who were younger, with a lower BMI, and lower blood pressure. Contrastingly, O’Malley et al. found that the association between dyslipidemia and GDM was only present in patients with obesity [3]. Our study indicates that there might be a high significance of lipid levels in our study cohort of Chinese women undergoing IVF/ICSI and in women with a low risk of GDM. While the median BMI in our study cohort was well within the normal range at 21.33 kg/m2, O’Malley’s study focused on women with at least one risk factor for GDM and the cohort had an overall obesity rate of 57.4%.
The 3D plots (Fig. 2a-b and Supplementary Fig. 5a-c), which display the relationship between LDL/HDL with other GDM risk factors on the incidence of GDM, show that in our cohort, the LDL/HDL ratio was an even stronger predictor for GDM incidence than BMI. However, the analyzed factors also interact with each other, meaning that there are complex underlying mechanisms related to the development of GDM. For example, women in our cohort with a high LDL/HDL ratio and a high pre-pregnancy fasting glucose level had a much higher risk of developing GDM, compared to women with low LDL/HDL and fasting glucose (Fig. 2a).
Concerning the association between lipids and GDM development, there are several explanations and hypotheses, but the exact mechanisms remain unclear. Eppel et al. found that high levels of TG were associated with insulin resistance as well as β-cell dysfunction [31], which are both factors that play a significant role in the pathogenesis of GDM. In combination, impaired β-cells cannot compensate for the increased insulin resistance, thus leading to higher plasma glucose levels and the development of diabetes. Another mechanism is an alteration in the lipid metabolism during pregnancy, whereby lipid levels increase at the beginning of pregnancy as a result of the anabolic metabolism and then are broken down again [32]; increased fatty acids and glycerol are transferred from the breakdown of adipose tissue to the placenta as well as to the liver for gluconeogenesis [33] – thus, producing more glucose and leading to GDM. Another case-control study found that women who developed GDM had lower pre-pregnancy LDL peak diameter size as well as lower HDL levels [34]. Smaller LDL particles are more prone to oxidation, leading to β-cell dysfunction, which could also contribute to increased GDM risk. Further research into the exact pathomechanisms is required to fully understand how lipids contribute to the development of GDM, especially in women undergoing IVF/ICSI, a subgroup of women with a very high GDM risk.
There are several study limitations, including that the family history of diabetes, the diagnosis of PCOS, and the use of medication, which are important risk factors for GDM, as well as pre-pregnancy HbA1c, were not recorded because this was a retrospective analysis of a previously prospective study focusing on IVF/ICSI outcomes. However, we have corrected for the biochemical diagnostic criteria for PCOS in the form of total testosterone concentration, as well as AFC and AMH in Model B of the multivariate logistic regression. Another limitation is that baseline blood tests were performed at different times before conception. As lipid levels can be significantly influenced by lifestyle factors such as diet and physical activity as well as uncontrollable factors, it could be beneficial to have several measurements from each study individual and evaluate their average. Furthermore, it is important to note that our study was a single-center study with only Chinese women, which is important because GDM has different prevalences in different regions and ethnicities. Therefore, the findings need to be studied in other cohorts to generalize our conclusions.
Strengths of this study include that this is the first study focusing on the effects of pre-pregnancy lipid levels on GDM incidence specifically in women undergoing ART. Furthermore, we measured four different lipid parameters and compared them, in addition to three different lipid ratios.



留言 (0)