Correlation between HE-OFC results and HE-specific IgE levels
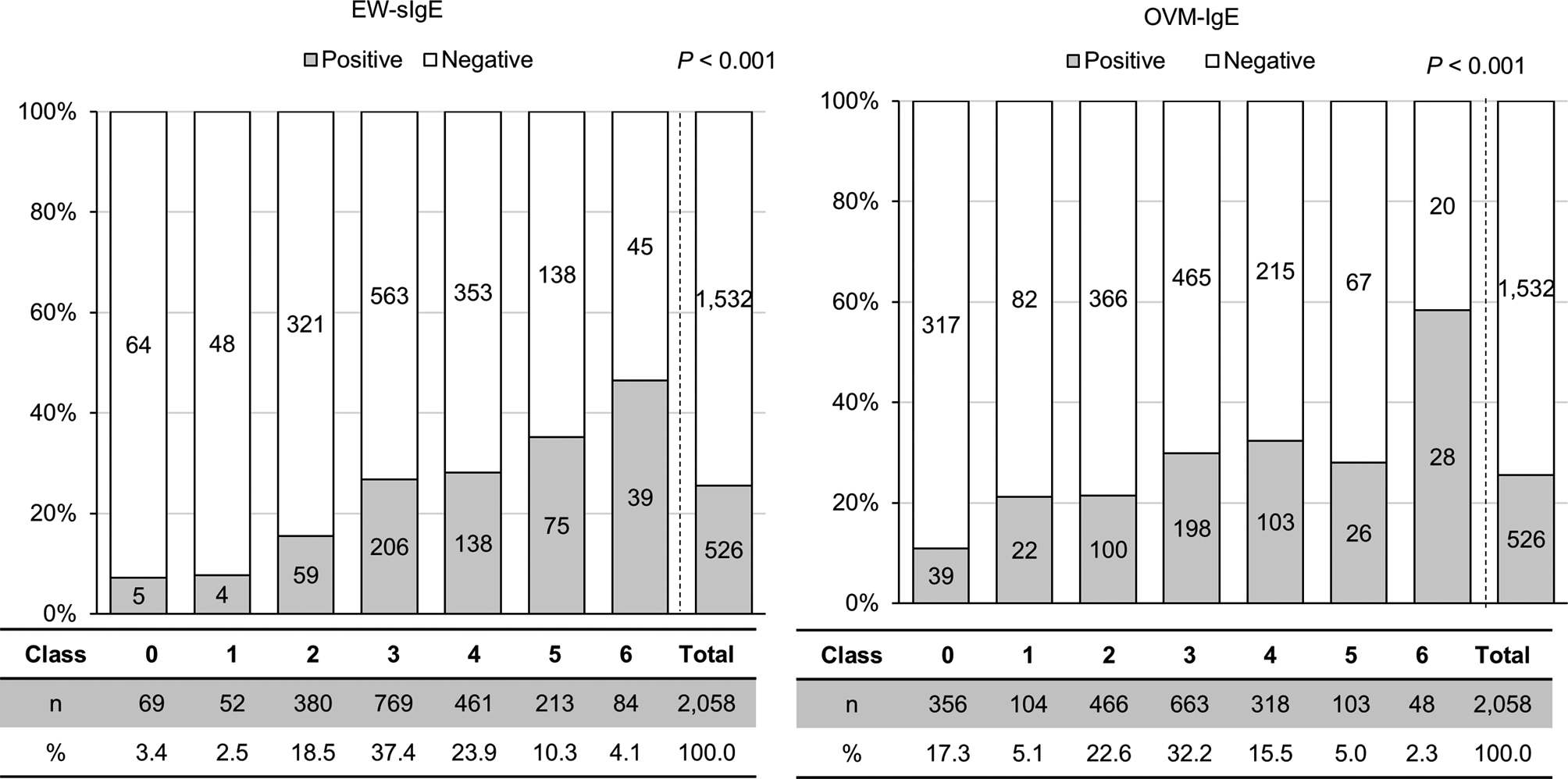
Of the 2,058 children with HE allergy, 526 (25.6%) showed positive reactions to HE in the HE-OFC (Fig. 1; Supplementary Data 3). There were no cases of anaphylactic shock. Higher serum EW-sIgE (P < 0.001) and OVM-sIgE (P < 0.001) levels were associated with positive OFC. Although 7.2% (5/69) of the children with EW-sIgE levels (class 0) presented positive reactions to HE, 2 were untreated, and 3 (multiple hives, 2; itchy mouth and nausea, 1) were successfully treated with antihistamines. Almost half (53.6%, 45/84) of the children with EW-sIgE (class 6) presented no allergic reaction in the OFC. Of these children, 5 could consume the full dose of boiled HE and 1 the medium dose. However, all 6 of these children presented an OVM-sIgE level below class 4 (class 4, 4; class 2, 1; and class 0, 1) and a disparity between EW and OVM-sIgE levels. Even among children included in OVM-sIgE class 6, 40.4% (20/48) were OFC negative. Only 2 children were tolerant to full-dose boiled HE, 4 to medium dose HE, 9 to low dose, and 5 to HE yolk. Supplementary Data 4 shows the characteristics of children with EW- or OVM- sIgE levels ≥ 100 kU/L (class 6).
Correlation between HE-OFC results and challenge doses
Of the 2,058 children, 621 (30.2%) received the low-dose OFC, 812 (39.5%) received the medium-dose OFC, and 625 (30.4%) received the full-dose OFC (Table 1). Allergic reactions were developed in 34.3% (213/621) of the children receiving the low-dose OFC, 23.5% (191/812) receiving the medium-dose OFC test, and 19.5% (122/625) receiving the full-dose OFC test. The frequency of the positive OFC test was higher in the low-dose OFC test than in the other tests (P < 0.001) (Table 1).
The median age of children undergoing the low-dose OFC test was lower than those in the middle-dose OFC and full-dose OFC (P < 0.001). Additionally, children in the low-dose OFC group presented higher levels of EW-sIgE (P < 0.001) and OVM-sIgE (P < 0.001), more histories of anaphylaxis (P<0.001), and higher active atopic dermatitis cases (P = 0.006) than the other groups. However, the frequency of wheezing history and immediate symptoms were similar (P > 0.05).
Comparison of OFC-positive and -negative subjects in total challenge doses
EW- and OVM-sIgE levels were higher in OFC-positive children than in OFC-negative children in every challenge dose test (Supplementary Data 5). Moreover, the OFC-negative children in the full dose OFC tests presented lower EW-sIgE and OVM-sIgE levels, with a median of 4.8 kU/L (IQR: 1.6–14.3 kU/L) and 1.6 kU/L (0.3–5.5 kU/L), respectively. Children undergoing each OFC test were older in the OFC-positive group than in the negative group; however, statistical significance was confirmed only in the low-dose OFC test (P = 0.010).
Of the children with a positive OFC (Table 2), children with a low-dose positive-OFC were younger when the OFC test was performed (P < 0.001) and showed higher EW- (P < 0.001) and OVM-sIgE levels (P < 0.001). Total IgE (P = 0.318), the frequency of wheezing history (P = 0.295), atopic dermatitis (P = 0.483), or immediate symptoms related to HE allergy (P = 0.664) were similar among age groups.
Both EW- and OVM-sIgE levels were substantially higher in positive-OFC children than in negative-OFC children in each total challenge dose (Supplementary Data 5). The cut-off values of EW- and OVM-sIgE indicating positive reaction for each OFC dose group were evaluated using ROC curves. The EW- and OVM-sIgE could not clearly predict OFC outcomes, with AUCs less than 0.7 in all OFC dose groups (Supplementary Data 6).
Can early low-dose OFC safely induce immune tolerance?
We focused on the low-dose OFC group because most children in this study initially underwent low-dose OFC. Although the low dose group included those who could consume low-dose or/and higher (medium- or full-dose) HE, this low-dose group showed more positive reactions and had higher EW- and OVM-sIgE levels than those who underwent the medium- or full-dose OFC test (Table 1). Of the children with class 0–2 EW- and OVM-sIgE levels, older children were more likely to develop allergic reactions to low-dose OFC (P < 0.001, Fig. 2A and B).
Even when the children developed positive reactions to low-dose OFC, we encouraged them to ingest a lower dose than the low-dose OFC to avoid the complete elimination of HE. In fact, 51% (317/621) of low-dose challenge cases could tolerate lower doses of HE, such as 1/50–1/200 of a cooked HE. Fewer children completely avoided HE with increasing age (P < 0.001, Supplementary Data 7). We hypothesized that intake of a small amount of HE may promote oral immune tolerance to HE in some older children.
We also evaluated the HE-OFC results in children (n = 304) who had not consumed HE in any form prior to the OFC and thus had not developed oral immune tolerance. The results were similar by age in each EW- and OVM-sIgE class group (Supplementary Data 8). Moreover, to investigate whether our dietary recommendation of such a trace amount of HE could indeed induce oral immune tolerance in the participants of this study, we compared the OFC results between complete and partial elimination of HE (Fig. 3). In the full dose, a partial elimination was likely to contribute to improving HE allergy, although there was no statistical difference.
In the low-dose OFC group, the ratio of positive OFC results was almost the same between complete and partial elimination groups (P = 0.800, 106/304 and 107/317, respectively). We also compared the OFC results between complete and partial elimination groups according to EW- or OVM-sIgE classes (classes 0–2, 3–4, 5–6) (Fig. 4). Although there were no differences (all P > 0.05), partial elimination tended to alleviate HE allergy in class 5 or more.
We expected cut-off values of EW- and OVM-sIgE to show positive low-dose OFC results in children who completely eliminated HE from their diet. EW- and OVM-sIgE could not predict OFC results because the receiver operating characteristic (ROC) curve indicated an area under the curve (AUC) < 0.7 (Supplementary Data 9). OFC was required for definite diagnosis in the partial removal group because EW- and OVM-sIgE levels could not be used as indicators. We then compared the results of medium-dose OFC (n = 812) in children who went through complete (n = 78) and partial (n = 734) elimination of HE (Supplementary Data 10). No apparent differences in OFC results between complete and partial elimination groups were observed, and EW- and OVM-sIgE did not contribute to the prediction of OFC results (Supplementary Data 11). These findings were consistent with the results of the low-dose OFC test.



留言 (0)