
記住我


Acute FPIES is characterized by profuse, repetitive vomiting that typically occurs 1–4 h (range: 30 min to 6 h) after ingestion of the trigger food (Tables 1, 2) [13, 14, 38]. Vomiting is often accompanied by lethargy, pallor, and diarrhea and, in rare severe cases, patients may experience hypotension, hypothermia, acidemia and methemoglobinemia. Symptoms may occur on first exposure to the trigger food or after a period of tolerance [13]. Like FPIAP and FPE, IgE-mediated skin and/or respiratory symptoms are typically absent in patients with FPIES.
Chronic FPIES occurs in the context of regular/ongoing ingestion of the trigger food. Presenting symptoms include intermittent vomiting, reflux, diarrhea and, in some cases, poor weight gain and failure to thrive (Table 1) [14, 39]. Symptoms resolve with elimination of the food trigger, but reintroduction induces an acute FPIES reaction (see “Diagnosis” for more details) [14].
Although FPIES typically presents in infancy, there have been increasing reports of FPIES in later childhood and adulthood, suggesting that onset of this non-IgE-mediated food allergy can occur throughout the lifespan [13,14,15,16,17,18]. The clinical presentation of FPIES in adults appears to vary somewhat from that in children, with abdominal pain and diarrhea being more common than vomiting in adult FPIES [15, 16, 18]. Case definitions and diagnostic criteria for FPIES are likely to be revised in the future to reflect the distinction in clinical presentation between adults and infants [17, 18].
EpidemiologyMost epidemiologic data regarding FPIES has focused on its presentation in children [16]. Cumulative pediatric incidence rates estimated from population-based cohort or national survey studies in the United States (US), Israel, Australia, and Spain range from 0.14% to 0.7% [16, 40, 41]. Although the presentation of FPIES in adults has been less well-studied, a US population-based survey reported an estimated lifetime prevalence of 0.22% in adults 18 years of age and older [42].
Chronic FPIES appears to be less common than acute FPIES, accounting for 10–15% of FPIES cases in infants [15]. The prevalence of chronic FPIES in adults is unknown. To date, there has been only one reported case of chronic FPIES in an adult patient [15].
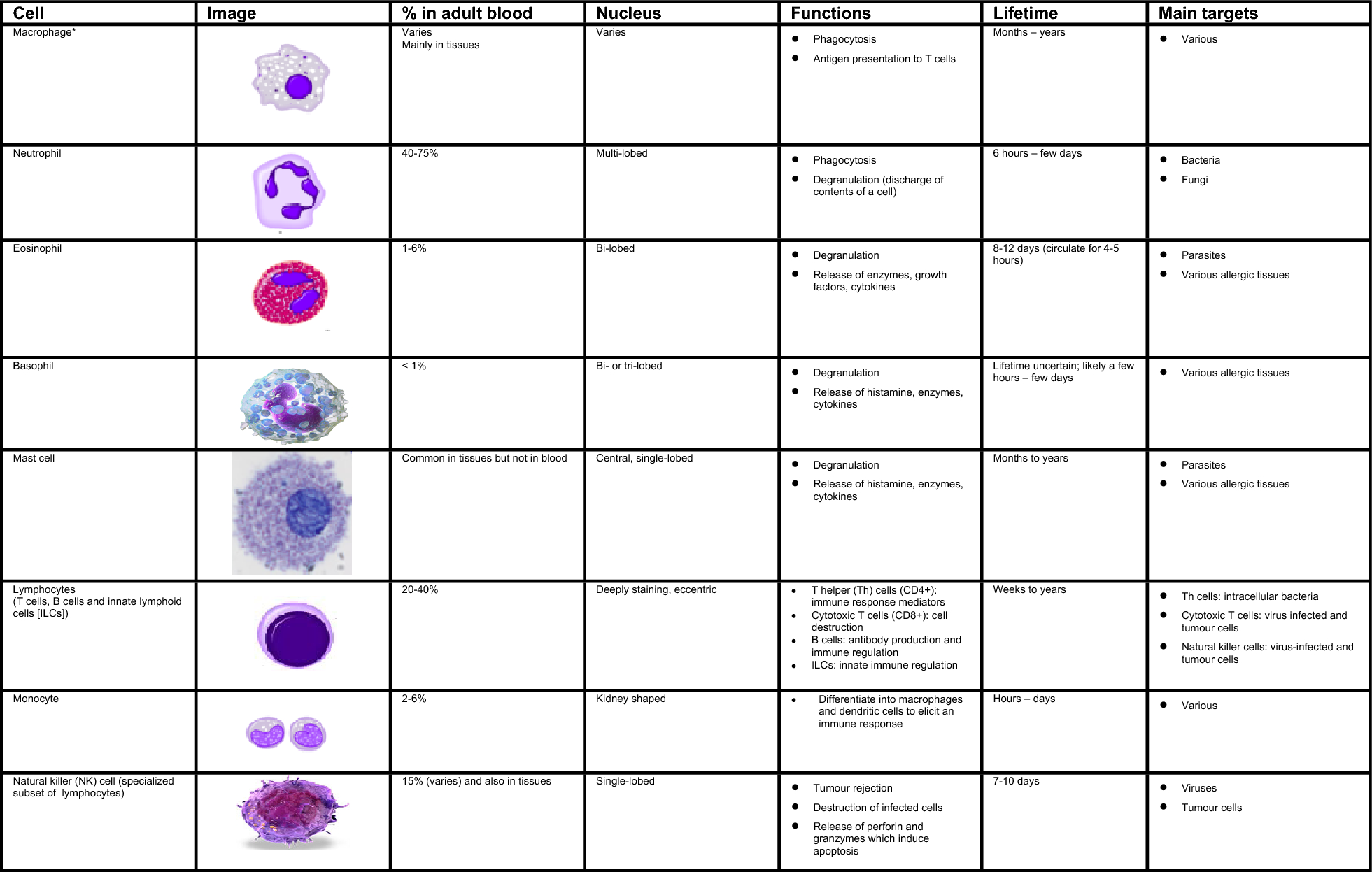
PathophysiologyThe pathophysiology of FPIES remains incompletely understood but it is thought to involve innate immune responses and Th17-mediated signaling, as evidenced by increased eosinophils in blood and stool samples from patients with FPIES as well as eosinophil infiltration in intestinal biopsy specimens [19, 43, 44]. Although biopsies are not typically performed in patients with FPIES, those that have been examined also show villous blunting and increased monocytes with tumour necrosis factor (TNF)-alpha expression [44].
Neuroimmune pathways have also been implicated in FPIES, as suggested by reports of successful outcomes using the selective serotonin receptor antagonist ondansetron to ameliorate FPIES reactions [19, 43, 44]. Serotonin is known to play a pivotal role in GI functions, including motility, secretion, and vasodilation. Overproduction and secretion of serotonin by enterochromaffin cells in the GI tract can lead to activation of vagal afferents that initiate the vomiting reflex [43]. Serotonin has also been shown to attract eosinophils into the GI tract [19, 43, 44].
There is also some evidence suggesting that alterations in the gut microbiome may play a role in the pathogenesis of FPIES [19]. However, at present, there is insufficient data to draw any definitive conclusions about the role of these alterations in FPIES development.
Food triggersEvidence suggests that most patients with FPIES react to a single food trigger, and that multiple food triggers are less common [40]. The list of common food triggers for FPIES varies considerably based on the age of the population studied and the specific feeding/dietary practices in the countries where studies were conducted [40, 41]. In adult cohorts with FPIES, fish and shellfish, followed by egg, are the most reported triggers [15, 40, 41]. The most common trigger foods reported in North American studies of pediatric cohorts include CM, soy, grains and egg, although meats, fish, fruits/vegetables, peanut and tree nuts have also been reported as triggers [13]. Interestingly, there have been growing reports of peanut- and tree nut-triggered FPIES since the implementation of guidelines for early introduction of these foods in infants to prevent IgE-mediated food allergy (see Primary prevention of food allergy: beyond early introduction article in this supplement for more details on these guidelines) [45,46,47]. A dramatic increase in FPIES provoked by hen’s egg has also been observed in Japan following the publication of the country’s food allergy prevention guideline updates, which recommended early introduction of hen’s egg in high-risk infants [48].
An Australian study of 230 infants with FPIES found that reactions during exclusive breast-feeding are uncommon, occurring in only 5% of cases [38]. This study also found that that the majority of infants with CM-triggered FPIES were able to tolerate elemental formula (only 1 of 28 reacted). Approximately 21% (6 of 28) reacted to extensively hydrolyzed formula, 47% (8 of 17) reacted to soy formula, and 70% (7 of 10) reacted to partially hydrolyzed formula.
Risk factorsAn Australian population-based cohort study of infants with FPIES found that 7% had a sibling with FPIES and 57% had a family history of atopy [38]. A US population-based study found significantly higher rates of atopic disease in children and adults with FPIES compared to those without FPIES [42]. Approximately, 5% of families in this study reported having multiple children with FPIES.
Eosinophilic esophagitis (EoE) (see EoE article in this supplement) has also been reported to be associated with FPIES. In another US population-based cohort study, 19% of children and 13% of adults with EoE had a history of FPIES compared to 0.48% and 0.19% of children and adults, respectively, in the general population [49].
FPIES also appears to be associated with other GI pathologies. A 10-year prospective study found the prevalence of irritable bowel syndrome, EoE, inflammatory bowel disease and celiac disease to be higher in adults with FPIES (12.1%, 4.7%, 3.7% and 2.8%, respectively) compared to the general population (4.6%, 0.1%, 0.3% and 0.7%, respectively) [50]. Another study found high prevalence rates of FPIAP (23.2%) and gastrointestinal reflux disease (GERD) (36.0%) in patients with FPIES [51].
At present, it is unclear if sex may predispose patients to FPIES development. In the pediatric population, some studies have noted a slight predominance of FPIES in males, while others have found no considerable differences between males and females [15, 41]. In contrast, an overwhelming female predominance of FPIES in adults has been observed [16]. This finding should be interpreted with caution given the small numbers of adult patients in case cohorts reported to date.
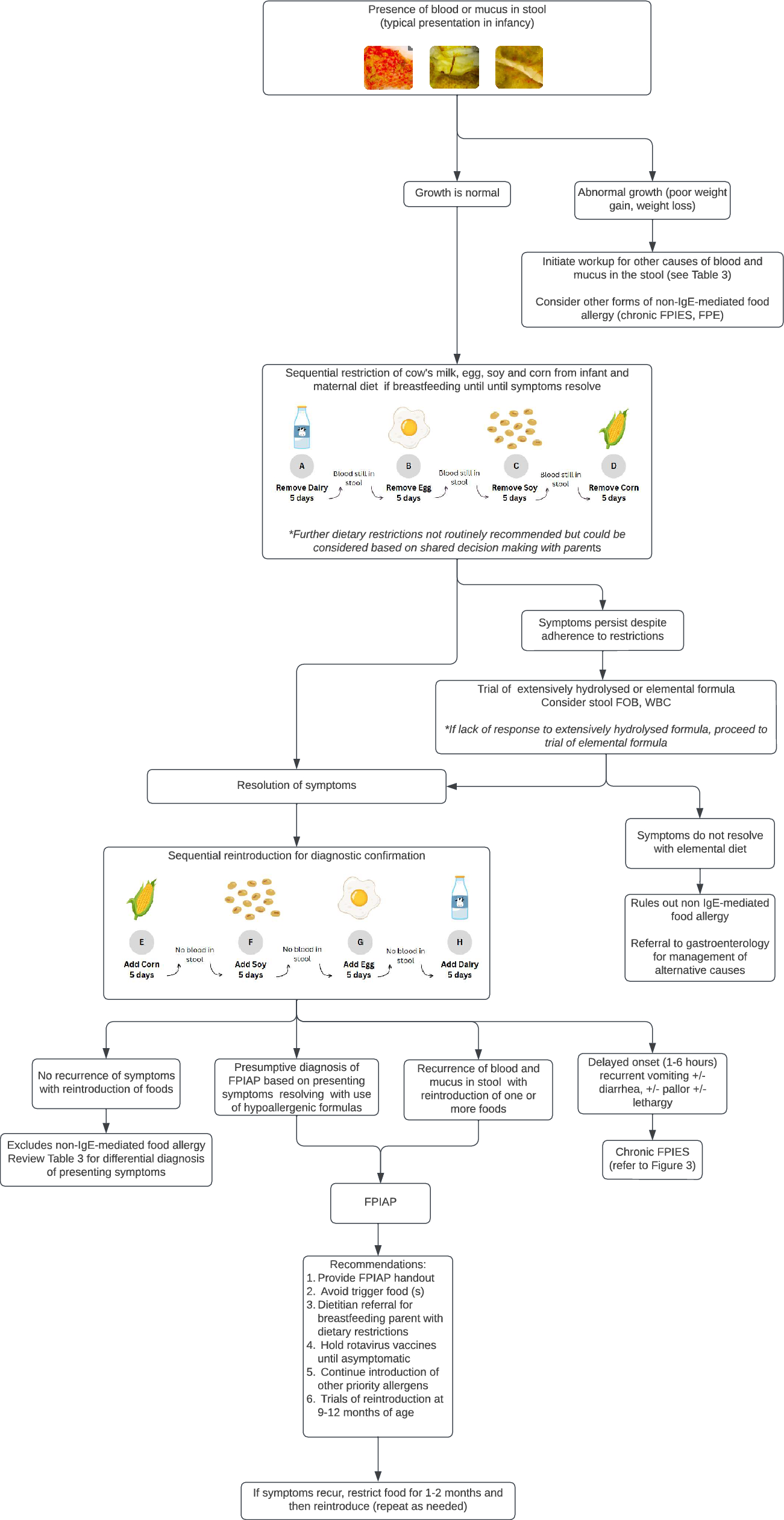
DiagnosisThe diagnosis of FPIES is based on recognition of the typical clinical features of the disorder (Table 1; Fig. 3). During the physical examination, it is important to assess growth parameters since growth is generally normal in acute FPIES, but failure to thrive and inadequate weight gain are often observed in those with chronic FPIES [2, 4, 29]. Reintroduction of the trigger food is required to confirm a diagnosis of chronic FPIES. Resolution of symptoms within 3–10 days after the elimination of the offending food(s) followed by acute recurrence of symptoms upon reintroduction have been reported as the most important criteria for the diagnosis of chronic FPIES [14]. However, without a confirmatory challenge, the diagnosis of chronic FPIES remains presumptive.
Fig. 3
Algorithm for the diagnosis and management of FPIES. FPIES food protein-induced enterocolitis syndrome, IgE immunoglobulin E, ED emergency department, IM, intramuscular, IV intravenous, PO oral, SL sublingual, PRN as needed
Laboratory tests, endoscopy or other investigations are generally not indicated in the work-up of patients with suspected FPIES, but they may be helpful if alternative diagnoses are being considered. If blood work is performed acutely, infants with FPIES often show evidence of leukocytosis, neutrophilia and methemoglobinemia [2, 13].
Skin prick testing and serum food-specific IgE testing are not required for the diagnosis of FPIES. However, because food avoidance can increase the risk of IgE-mediated food allergy in susceptible individuals, these tests may be considered by the treating allergist prior to food reintroduction to gauge the patient’s risk of IgE-mediated allergy.
Differential diagnosisSeveral allergic, infectious, GI, and immunologic disorders need to be considered in the differential diagnosis of FPIES (Table 3) [3, 9, 18, 52]. Acute viral gastroenteritis is the most common diagnosis of exclusion for acute FPIES. Unlike FPIES, viral gastroenteritis is not associated with a specific food trigger and vomiting is often accompanied by diarrhea and fever [52]. Chronic FPIES with intermittent vomiting and/or diarrhea leading to failure to thrive has a broader differential diagnosis. In fact, FPIAP, FPE and EoE can present with similar symptoms to chronic FPIES. However, in these disorders, reintroduction of the food trigger is not associated with acute FPIES symptomatology [52].
ManagementIn general, patients with FPIES should be referred to allergy/immunology for assessment, evaluation, and ongoing care (Fig. 3) [13, 14]. The standard of care for FPIES management is avoidance of the food trigger followed by reintroduction under specialist supervision (during a formal oral food challenge [OFC]) to see whether the disorder has resolved. Some practitioners may consider gradual home reintroduction in patients with prior mild reactions to large amounts of the trigger food (e.g., few episodes of vomiting, no or minimal lethargy) and who recovered at home without the need for healthcare intervention [52].
The likelihood of spontaneous resolution after a period of avoidance is lower in adults compared with children. Therefore, in adult patients, shared decision-making should be used to determine whether to proceed with reintroduction and OFC [16].
Treatment of acute episodesThe treatment of acute FPIES symptoms is supportive and tailored to the severity of symptoms [17, 18, 43, 53]. In the setting of mild reactions with no significant lethargy or signs of hypotension, enteral ondansetron and oral rehydration at home can be considered. A single dose of intravenous (IV) or intramuscular ondansetron (0.15 mg/kg; 2 mg for patients weighing 8–15 kg, 4 mg for those weighing 15–30 kg and 8 mg for those weighing > 30 kg) has also been shown to be effective for resolving vomiting and reducing the risk of dehydration in acute FPIES [13, 54].
In more severe cases with dehydration and hypotension, IV fluid boluses (10–20 mL/kg of normal saline) and IV corticosteroids (e.g., methylprednisolone 1 mg/kg to a maximum of 60–80 mg) are recommended [13, 17]. However, it should be noted that there are currently no studies demonstrating the efficacy of IV corticosteroids in the treatment of acute FPIES reactions.
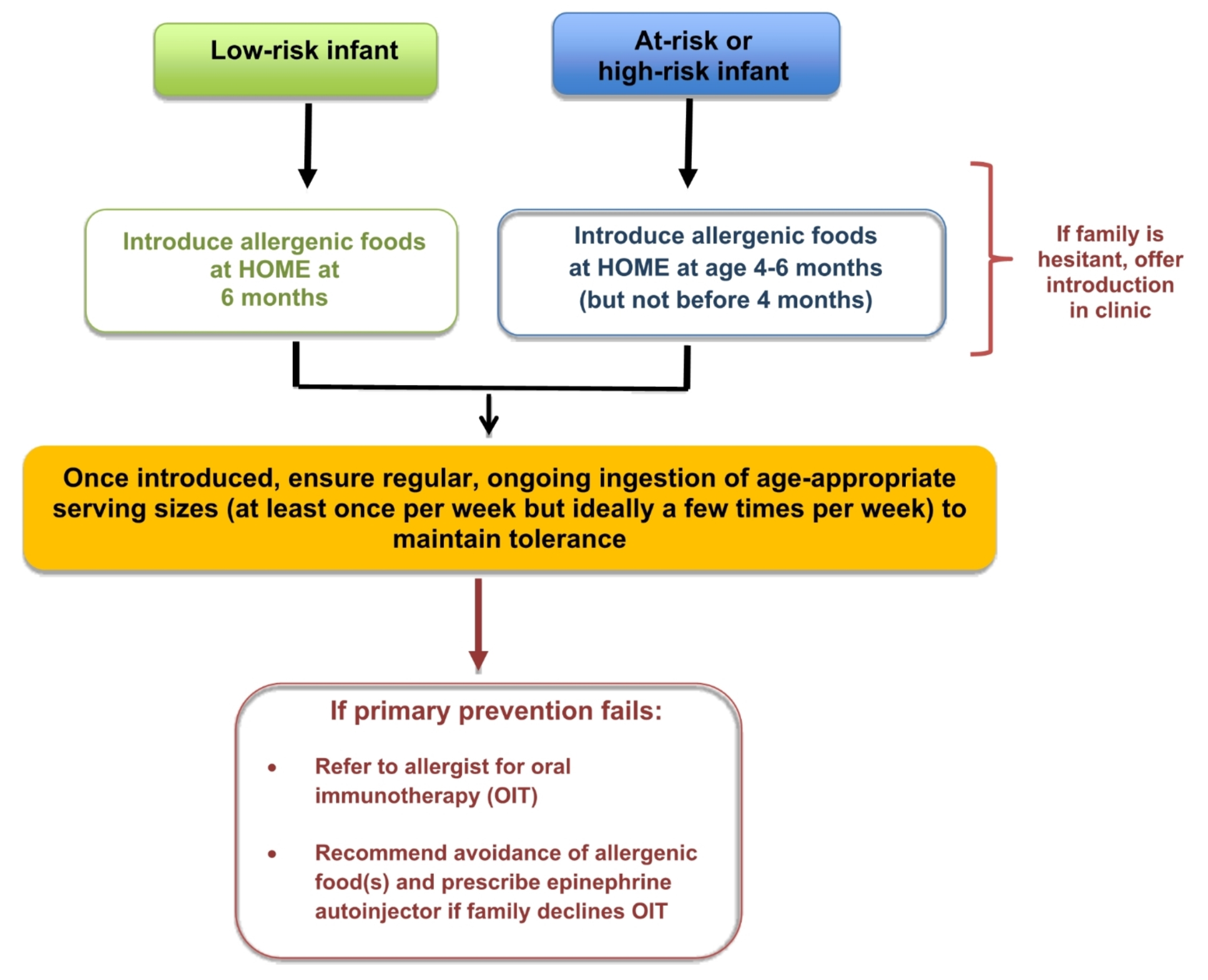
At-home management (post-acute event)As mentioned earlier, the primary management of FPIES consists of avoidance of the trigger food. Avoidance of other common FPIES triggers or allergenic foods during infancy is not recommended [13]. Current guidelines for the prevention of IgE-mediated food allergy (see Primary prevention of food allergy: beyond early introduction article in this supplement) emphasize the importance of early introduction of commonly allergenic foods at around 6 months of age (and not before 4 months), especially if the child is at risk for IgE-mediated allergy [55, 56]. Delays in the introduction of these foods increase the risk of developing IgE-mediated food allergy.
In contrast to IgE-mediated allergy, there is no need to avoid food products with precautionary (e.g., ‘may contain’) labelling and, in most cases, no need for maternal elimination of trigger foods in breastfed infants with FPIES [13].
Patients with CM- or egg-triggered FPIES who can tolerate extensively heated forms of these foods should be encouraged to continue consumption of these heated forms [17, 57]. In fish/shellfish-FPIES, there is evidence suggesting that some patients can tolerate alternate types of fish/shellfish other than the offending one [58, 59].
Patients and families should be counseled on the signs and symptoms of FPIES reactions and, in the event of an accidental exposure, how to monitor for signs and symptoms of dehydration and hypotension that should prompt emergency evaluation [43]. Patients/parents should also be provided with a letter to bring to the emergency department (ED) that explains what FPIES is and provides recommendations for treatment [53]. An example of an ED letter is provided in Fig. 4.
Fig. 4
Example of pediatric ED letter. Letter adapted by Dr. Victoria Cook based on ED letter (for children) available on the International FPIES Association website at https://fpies.org/ (see “Resources” section)
Patients/families may also be provided with a prescription for ondansetron to be used as needed in the case of intractable vomiting upon accidental exposure to the food trigger [43, 53, 60]. Ondansetron has been associated with QT prolongation, so caution is recommended in patients with long-QT syndrome or other cardiac disease, or in those using other QT-prolonging medications [43, 53, 60].
An epinephrine autoinjector is not indicated for the treatment of FPIES as it has no effect on vomiting or other FPIES symptoms [13]. However, in cases where the diagnosis is unclear and there is suspicion of IgE-mediated food allergy, an epinephrine autoinjector could be prescribed until the patient is evaluated by an allergist. Epinephrine will not be harmful during an FPIES reaction.
PrognosisThe prognosis of pediatric-onset FPIES is good, with most cases resolving by school age. A large retrospective review of over 400 children with FPIES found resolution rates of 35% by age 2 years, 70% by age 3 years, and 85% by age 5 years [61]. Evidence suggests that resolution rates and median age of resolution vary by type of FPIES trigger. CM-triggered FPIES has been reported to resolve earlier than FPIES triggered by fish or egg [40]. This is likely related to timing of food introduction as CM is generally introduced at an earlier age than other foods and, thereby, tolerance may be acquired earlier. Patients with fish-FPIES appear to have the lowest rates of resolution and the highest median ages of resolution. In egg-FPIES, evidence suggests that tolerance to cooked egg is achieved earlier than to raw egg [40].
There is limited data on resolution rates in adult-onset FPIES. In a prospective study that followed 107 ad
留言 (0)