The measurement of blood eosinophil count, the most established predictive biomarker for targeted biologic treatment response [13], is an important step towards the phenotypic characterization of patients with asthma and assessing targeted biologic therapy eligibility [16]. This large, retrospective study provided insight into the real-world prevalence of blood eosinophil count testing for patients with asthma in the US. Results of this study show that regardless of exacerbation frequency or HCP type, approximately 70% of patients are likely to have blood eosinophil counts ≥ 150 cells/µL, making them potentially eligible for targeted biologic therapy. Furthermore, more than one-third of patients could be considered to be in a highly responsive subgroup for this therapy, with blood eosinophil counts ≥ 300 cells/µL [8, 17, 18]. Although Allergists or Pulmonologists are more likely to perform blood eosinophil count tests compared with other HCPs, particularly in patients with frequent exacerbations, only two-thirds of patients are being tested, which could limit access to targeted biologic therapy. Overall, these results highlight that despite patients having a high burden of disease, indicated by the common comorbidities, exacerbation frequencies and high OCS dependencies, blood eosinophil count tests are suboptimal.
Of the 400,254 patients included in this study, over three-quarters (77%) were cared for by a PCP, with 17% in the care of a specialist Allergist/Pulmonologist. Overall, demographics in this study population were consistent with previous asthma real-world studies [10, 16, 17], with a mean age of 51 years and a higher predominance of asthma in females (70.8%). While baseline demographics and clinical characteristics were generally similar between patients by exacerbation frequency, clear differences were seen when analyzed by HCP type. Patients with asthma under Allergist/Pulmonologist care were typically older and had more frequent exacerbations throughout the study compared with those under PCP or other HCP care. This is potentially a reflection of the time it takes for patients with severe asthma to be referred to a specialist for treatment and the severity of their disease once referred. Accordingly, patients under the care of an Allergist/Pulmonologist also had higher comorbidity index scores and more frequently had the top 10 comorbidities assessed in the study, with over half of patients in this subgroup having comorbid hyper-tension. Additionally, patients under the care of an Allergist/Pulmonologist had the greatest use of other asthma medications (ICS, OCS, SABA and SAMA) in the baseline and follow-up periods compared with patients under the care of a PCP or other HCP. Together, these results suggest that patients with a greater burden of asthma-specific and unrelated comorbidities may have asthma that is more severe and difficult to treat and are more likely to be referred for specialist care.
Analysis of demographics by HCP types also highlighted potential differences in access to healthcare among racial and ethnic groups. Observation of trends among ethnic subgroups highlighted that fewer African American and Hispanic/Latino patients received specialist Allergist/Pulmonologist care than Caucasian patients. This is consistent with previous reports of disparities in access to specialty asthma healthcare among African American and Hispanic/Latino communities and may result in the under-prescription of targeted asthma therapy to these patient subgroups, along with overall increased morbidity [19].
Although patients under Allergist/Pulmonologist care more frequently had blood eosinophil counts performed during the baseline or follow-up periods, compared with other HCPs, approximately one-third of all patients did not have the test performed. An unexpected finding in the current study was that within the subgroup populations, a slightly lower proportion of patients in the Allergist/Pulmonologist and PCP subgroups (64% and 63%, respectively) had a blood eosinophil count or CBC count test on follow-up, compared with patients in the other HCP provider subgroup (68%). The other HCP subgroup included 98 different specialties with a preponderance of hospital-based specialist services; however, it is unclear why this group had the lowest proportion of patients with blood eosinophil counts at baseline, but amongst the highest rates of testing at follow-up. Testing was even less frequent in patients who were under the care of a PCP: between 32% and 44% of patients did not have a blood eosinophil count test performed. Additionally, 3–45% and 25–35% of patients with frequent exacerbations did not have a blood eosinophil count ordered in the baseline and follow-up periods, respectively, across HCP subgroups. Consequently, up to approximately half of patients with frequent exacerbations who may be eligible for targeted biologic therapies are not being assessed for eligibility. It is important to note that the proportion of patients determined in this study to have had eosinophil counts measured may be an underestimation, due to the limitations of the analysis or measurement of eosinophilic inflammation by alternative methods such as with fractional exhaled nitric oxide levels. However, clinicians who use these alternative testing strategies may also check blood eosinophil counts.
Although associated with greater healthcare resource use for patients [20], blood eosinophil count testing and referral to specialist care settings are important to ensure that patients with severe asthma are not being undertreated or are over-reliant on OCS use [21]. Consequently, current GINA recommendations suggest that patients with asthma under specialist care undergo blood eosinophil count/CBC testing, among other parameters [1]. Overall, there was no difference in blood eosinophil count tests ordered between patients with frequent and infrequent exacerbations; in patients with frequent exacerbations, this finding was despite half of patients using OCS during baseline and nearly all patients using OCS during follow-up, highlighting the unmet needs of these patients. Moreover, for patients under the care of all HCP types, there was an increase in other asthma medication use including ICS, OCS, SABA and SAMA from baseline to follow-up. Implementing blood eosinophil count testing in primary care could prove useful in identifying a subset of patients who would benefit from referral to an asthma specialist and targeted treatment. This is particularly evident in the context of the large proportion of patients receiving care with a PCP (77%) or other HCP (7%) compared with specialist care (16%). Consequently, this represents a considerable population of patients who could benefit from earlier blood eosinophil count testing and subsequently specialist care and/or targeted treatments [1]. PCP care is important for patients with asthma to reduce rates of uncontrolled asthma due to poor adherence; this should be supported in tandem with seeking appropriate specialist care [22]. Future research should also consider analyzing eosinophil testing rates by patient outcomes.
Regardless of HCP type, more than half of patients had a maximum blood eosinophil count ≥ 150 cells/μL, with higher counts more commonly in patients who experienced frequent exacerbations. Specifically, approximately half of patients with frequent exacerbations in the follow-up period had maximum blood eosinophil count values ≥ 300 cells/µL. This is consistent with previous evidence suggesting patients with moderate-to-severe asthma are more likely to present with an eosinophilic phenotype compared with patients with mild asthma [23]. This suggests that a considerable proportion of patients with asthma are not receiving tests despite potentially being eligible for additional treatment options available to them [1]. Accordingly, even though a larger number of patients under Allergist/Pulmonologist care received targeted biologic therapy compared with other HCPs, the absolute proportions were low (~ 2%) during the baseline and follow-up periods. However, as this study did not require evidence of targeted biologic therapy use for patient selection, this may have resulted in the underestimation of the prevalence of targeted therapies, making causality difficult to establish. Although conclusions cannot be definitively drawn from this study regarding the levels of targeted biologic therapy use by HCP subgroups due to the study design, this finding may reflect that some biologic therapy treatments for severe (eosinophilic) asthma including mepolizumab [24], benralizumab [25], reslizumab [26], and dupilumab [27] were only approved during the study period. Omalizumab, however, was approved before the study period and was found to be the most frequently used biologic. Given serum IgE levels are tested to guide omalizumab dosing in patients with severe asthma and blood eosinophil count is not required for treatment, this may have resulted in a lower prevalence of blood eosinophil count testing than may be expected if this study was repeated following these more recent approvals. The biologic approvals were based on demonstrated efficacy in reducing exacerbation rates, reducing OCS use and improving HRQoL in both clinical trials and real-world settings [6,7,8,9,10,11, 14, 17, 28]. Greater efficacy (reduction of asthma exacerbation) of asthma biologics in patients with higher blood eosinophil counts has also been demonstrated in clinical studies [7, 8, 29,30,31].
Overall, these data support the recent study from Heaney et al., [4] which reported that a larger proportion of patients with severe asthma may have an eosinophilic phenotype than previously suggested. As per the GINA guidelines, blood eosinophil counts can vary over time and repeated testing measures are required to ensure accurate phenotyping of eosinophilic asthma [1]. The Heaney et al. study considered patients with asthma who had a maximum blood eosinophil count of ≥ 300 cells/μL or blood eosinophil count of ≥ 150–300 cells/μL with OCS use or a combination of comorbidities classified as eosinophilic; within this study, 36–59% of patients had a maximum blood eosinophil count ≥ 300 cells/μL, with a further 22–31% having a maximum blood eosinophil count ≥ 150–300 cells/µL [4]. In the present study, the findings were similar, with the proportion of patients who had a maximum blood eosinophil count of ≥ 300 cells/µL ranging from 36 to 53% across patients and HCP subtypes at baseline and from 38 to 59% across exacerbation frequency and HCP subtypes during the follow-up period.
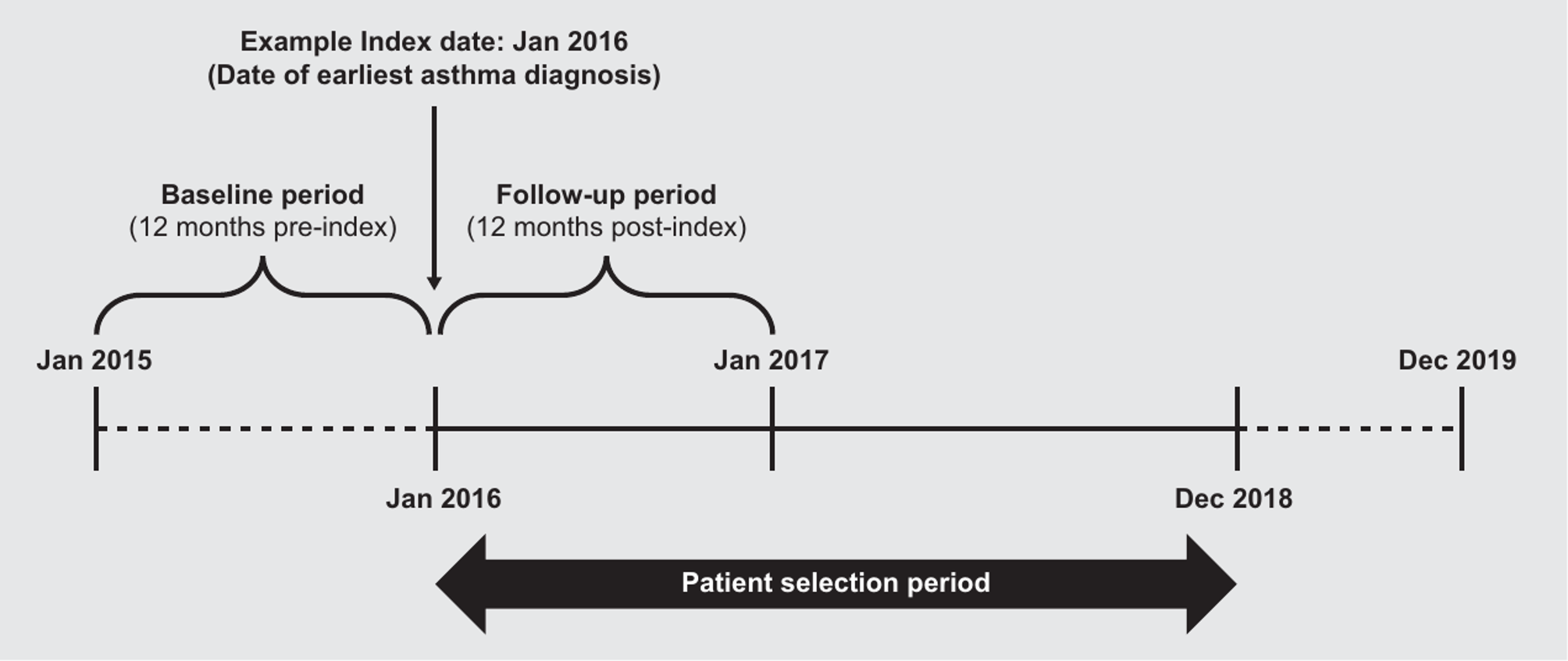
There are several inherent limitations to this database-based study, which should be considered when interpreting the results. First, this study is limited to only those patients seeking care with providers covered by the Explorys® Universe Database system. As a consequence, the results may not be generalizable to all patients with asthma, for example, most patients within the database were located in the North Central region of the US, so these results may not be representative of a more broadly distributed population of patients with asthma in the US. Additionally, if testing was performed outside of the integrated delivery networks which provide data to Explorys®, the results may not have been captured. Second, the study was claims-based in nature and may include coding limitations and/or data entry errors. Third, these data were calculated as aggregate results, therefore determining how many patients who were not blood eosinophil count/CBC tested during the baseline period then subsequently tested during the follow-up period was not possible. Fourth, this study period concluded in 2019, therefore these data may not capture the current prescribing levels of the more recently available targeted asthma therapies, and may not reflect GINA guideline changes including the requirement of patients to have blood eosinophil count tests. Furthermore, as mepolizumab, benralizumab, dupilumab, and reslizumab were newly approved at the time of the study period, the data captured here may not reflect the current levels of blood eosinophil count testing used by physicians to determine eligibility for these now well-established biologic therapies. Fifth, for patients who experienced comorbidities such as atopic dermatitis, COPD or rheumatoid arthritis, the use of CBCs with differential to assess and manage these conditions may make blood eosinophil counts more readily available. Similarly, since biologics were approved for other conditions such as atopic dermatitis during the study period, prescriptions for targeted biologic therapies may not be exclusively for severe asthma. Sixth, while availability of laboratory data and evidence of outpatient utilization were required for inclusion in the study, the availability of prescribed medication for inclusion in the study was not required. Therefore, asthma medication utilization is likely an underestimate. However, this underreporting is unlikely to differ by HCP type. Finally, blood eosinophil counts may have been assessed outside of the study period or through another method not captured by this study design; however, while analysis of blood eosinophil counts are a recent development, an eosinophilic phenotype (≥ 150 cells/µL) appears to be associated with increased healthcare usage, making it likely that a high proportion of these were captured in this study [20].



留言 (0)