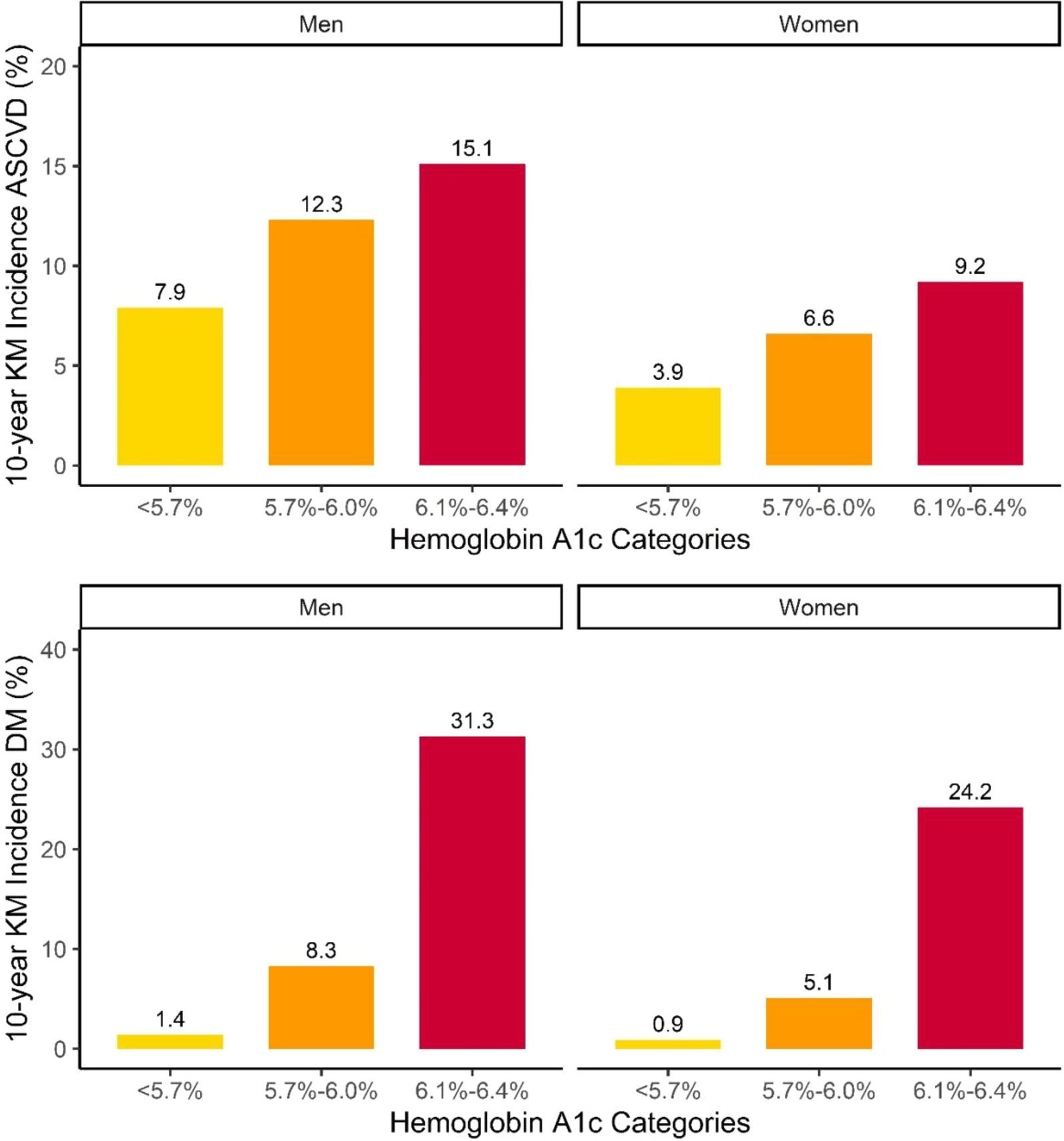
This study examined the association of low (HbA1c 5.7–6.0%) or high prediabetes (Hb6.1–6.4%) in women and men with new onset DM and ASCVD as well as the impact of increasing waist circumference (or waist to hip ratio) on new onset DM. Our analyses demonstrate that ASCVD risk was significantly increased in both low and high prediabetic groups in men and meaningfully increased in high prediabetic women. The Cox regression analyses confirmed that prediabetes contributed independently, at least moderately, to this increase in risk and this adverse effect was more evident in those with high versus low prediabetes. Our interpretation is that it is worthwhile to alert clinicians to the increased ASCVD risk that both men and women with high prediabetes face and this should encourage preventive therapies aimed at lowering lipids and blood pressure in these subjects.
However, it is the variance in conversion rates to DM amongst our subjects that may be the most noteworthy finding of our study. In normoglycemic subjects, although this rate increased as abdominal obesity, estimated by either waist or waist to hip ratio, increased, the absolute incidence remained low- 1.4% in men and 0.9% in women. By contrast, the conversion rate was substantially higher in all subgroups of prediabetics. In high prediabetics, the conversion rate to DM was striking- 31.3% in men and 24.2% in women, rates that were almost threefold greater than in low prediabetic men and women. The interaction of abdominal obesity with HbA1c as predictors of DM was also noteworthy. In men with high HbA1c prediabetes, the propensity to develop diabetes was substantial even in the lowest quartile of waist circumference. In women with high HbA1c prediabetes, in the two lowest quartiles of abdominal obesity, the risks were about half that in men. In the two higher quartiles, however, while less, the rates of conversion to diabetes in the high prediabetic women approximated those of men. By contrast, in both low prediabetic men and women, although the conversion rates to DM increased as abdominal obesity increased, the absolute rates were substantially less than the comparable high prediabetic groups. These appear to be clinically meaningful differences, which should inform the choice of prevention strategies in research studies and clinical care. Finally, since our findings were virtually identical, whether abdominal obesity was estimated based on waist circumference or waist to hip ratio, the simpler metric- waist circumference- would seem to be sufficient in clinical care.
Lifestyle interventions combining exercise and diet should remain the primary interventions to reduce the rate of progression from prediabetes to diabetes and should be broadly applied in all patients with prediabetes [10. 11] But there are now multiple pharmacologic approaches to delay progression to diabetes from prediabetes, ranging from metformin to glucagon-like peptide- (GLP-1) receptor antagonists, which differ in the evidence base justifying their application, potential risk, and actual cost [12,13,14,15] There are considerable data that metformin can reduce the rate of diabetic progression from prediabetes. However, presently, its use is prioritized for those with a BMI > 35 [16]. Our data suggests this could be reconsidered, as, certainly in males, a HbA1c 6.1–6.4%, whatever the level of abdominal obesity, is associated with a markedly elevated rate of conversion of prediabetes to diabetes. Similarly, the evidence that pioglitazone can significantly reduce progression to DM should not be lost sight of [17].
To be sure, amongst those with normal HbA1c, the relative risk of DM does increase steadily as abdominal obesity increases. Nevertheless, the absolute 10-year risk is just above 3% in those within the highest quartile of obesity. Accordingly, therapies to reduce weight that are associated with significant cost or potential risk, such as the glucagon-like peptide-1 (GLP-1) receptor agonists, should not be prioritized for these individuals. Rather, our results suggest the potential balance of benefit and risk appears most opportune in individuals with prediabetes with HbA1c between 6.1 and 6.4% and higher levels of abdominal obesity where the risk of conversion to DM over 10 years exceeds 20%.
Waist circumference is a reliable indicator of visceral adiposity. Visceral adipose tissue includes omental, perinephric, and perimesenteric fat, which hypertrophy as fat mass increases. This visceral fat mass expansion underlies insulin resistance, the progressively reduced ability of systemic cells to internalize glucose because intracellular transduction of the insulin signal is impaired with reduced cell surface expression of glucose transport proteins [18]. Insulin resistance is also a necessary precursor to the development of type 2 DM. Beyond impaired glucose homeostasis, numerous other abnormalities develop. Insulin resistance worsens as adiponectin levels decrease and resistin levels increase [19].The insulin resistant adipose tissue becomes a source of inflammatory adipokines (e.g., interleukin-6, tumor necrosis factor-alpha, transforming growth factor-beta) which potentiate adipose tissue and systemic inflammatory tone [20].In addition, the adipose tissue becomes infiltrated with inflammatory white cells which boost the inflammatory response. When visceral adipose tissue becomes insulin resistant, insulin no longer inhibits hormone sensitive lipase and free fatty acid is constitutively released [21]. These free fatty acids are taken up by the liver and can be reassimilated into triglycerides and packaged into very large density lipoproteins (VLDL), which are synthesized and secreted at an increased rate by hepatocytes [22, 23].The VLDL particles, which are secreted into plasma are inadequately lipolyzed since lipoprotein lipase is inhibited to a significant degree by reductions in its activator (apoCII) and elevations in its inhibitor (apoCIII), manifestations of insulin resistance [24]. As VLDL levels rise, so does the availability of triglyceride-enriched lipoproteins (remnant lipoproteins). Like LDL, remnant lipoproteins are atherogenic. [25] Secondary to increased cholesterol ester transfer protein activity and increased loading of LDL and HDL with triglyceride, there is a substantial rise in the number of LDL particles and a reduction in HDL particles leading to development of the so-called atherogenic lipid triad (high triglyceride and lipoprotein remnant levels, high levels of LDL particles, and low levels of HD) [26].Completing the pathophysiological cycle, Faraj and her colleagues have shown uptake of LDL particles by adipocytes results in increased production of proinflammatory factors, further provoking the development of insulin resistance [27]. Increased visceral adipose tissue is clearly an independent hazard for the development of both ASCVD and type 2 diabetes mellitus.
Our findings also, potentially, open an avenue to resolve the paradox that while DM substantially increases the risk of ASCVD, randomized clinical trials did not demonstrate that intensive control of hyperglycemia substantially reduced the risk of ASCVD [28]. ASCVD risk is multiplied by DM. However, although the effect is much less pronounced, ASCVD risk is also increased significantly with prediabetes. Could it be that the hyperglycemia of prediabetes significantly accelerates progression of ASCVD, although not to the same degree as the more extreme hyperglycemia of DM? [3,4,5] By controlling serum glucose earlier and more stringently, might it be possible that the adverse effects of the hyperglycemic milieu (increased binding of receptors of advanced glycated end products, increased adduct formation between enzymes and proteins with glucose, glycosylation of lipoproteins, impaired HDL functionality, endothelial dysfunction, abnormal macrophage function) would be attenuated enough to reduce rates of atherogenesis? [29,30,31,32,33] It may well be that, once established, atherosclerotic disease cannot be reversed or stabilized by treatment of the hyperglycemia [28]. Nevertheless, it seems anatomically and pathophysiologically plausible that more intensive treatment of hyperglycemia in prediabetes, when anatomic disease, at least on average, is not advanced, might be clinically beneficial notwithstanding this was not the case in patients with established DM, in whom more advanced and extensive disease was likely present. We concede this is only a hypothesis, but we suggest it is one worth testing in a randomized, prospective clinical trial.
An important limitation in our study is the absence of data on insulin resistance. Unfortunately, this was not measured routinely in the subjects in UK Biobank and therefore, we cannot examine its role as a determinant of the risk of DM.
In summary, we observe that the absolute risk of ASCVD is increased in prediabetic subjects with HbA1c 5.7–6.0% but the increase in both men and women is more striking in prediabetic subjects with HbA1c 6.1–6.4%. At the same time, men and women with pre-diabetes are at a substantial risk of conversation to DM. This underscores the importance of preventing the development of DM and efforts to reduce cardiometabolic risk through optimizing multiple risk factors in both categories of prediabetes. Risk modification therapies should be targeted at those with highest risks based on HbA1c and abdominal obesity.


留言 (0)