
記住我
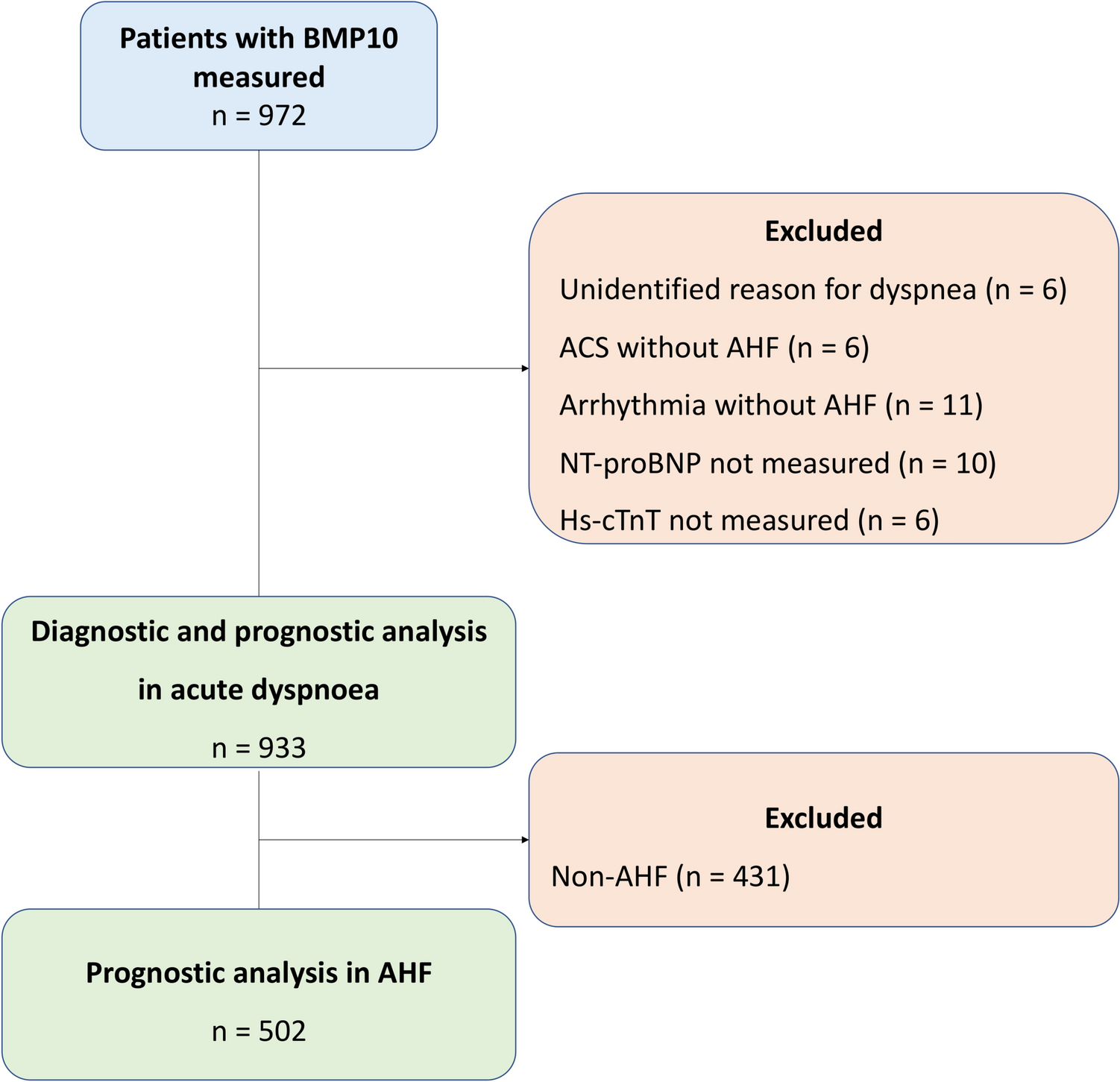
Among 972 consecutively enrolled patients with BMP10 concentrations available, 933 patients (96%) met the criteria for inclusion (Fig. 1). The median age of the patients was 76 (64–83) years, 45% were women, about a third had a history of heart failure, and 30% had atrial fibrillation (Table 1).
Table 1 Baseline characteristics of the patients presenting to the emergency department with acute dyspnea stratified by the presence or absence of acute heart failureCentral adjudication revealed AHF as the cause of acute dyspnea in 502 (54%) patients.
Plasma BMP10 in the study populationPlasma BMP10 concentration in patients with AHF was higher than in non-AHF patients (3.34 [2.55–4.35] vs 2.04 [1.74–2.45] ng/mL, p < 0.001, respectively). Among the different AHF phenotypes, acute coronary syndrome-associated AHF patients had the lowest plasma BMP10 concentration (2.76 [2.15–3.40]), whereas patients with cardiogenic shock had the highest plasma BMP10 concentration (4.85 [4.15–6.85] ng/mL, p < 0.001, Fig. 2). Patients with heart failure with reduced ejection fraction (HFrEF) had higher plasma BMP10 concentration as compared to patients with heart failure with preserved ejection fraction (HFpEF, Fig. 3).
Fig. 2
Plasma BMP10 concentration across the different Acute Heart Failure phenotypes. ACS acute coronary syndrome, AHF acute heart failure, BMP10 Bone Morphogenetic Protein 10, RV right ventricular. *Significant difference between ACS-complicated AHF (reference phenotype) and the corresponding phenotype (p < 0.05)
Fig. 3
Plasma BMP10 concentration across the different left ventricular ejection fraction phenotypes of Acute Heart Failure. AHF acute heart failure, BMP10 Bone Morphogenetic Protein 10, HFmrEF heart failure with mid-range left ventricular ejection fraction, HFpEF heart failure with preserved left ventricular ejection fraction, HFrEF heart failure with reduced left ventricular ejection fraction, LFEF left ventricular ejection fraction
BMP10 concentrations were comparable across the different diagnostic categories in the non-AHF group (p > 0.05, Supplemental Table 1).
Diagnostic performance for AHFThe diagnostic accuracy of plasma BMP10 levels in identifying AHF, as measured by AUC, was high (0.85, 95% CI 0.82–0.87), significantly higher versus hs-cTnT (0.79, 95% CI 0.76–0.82, p for comparison < 0.001), but significantly lower versus NT-proBNP (0.91, 95% CI 0.90–0.93, p for comparison < 0.001). When combined with NT-proBNP, BMP10 did not improve the diagnostic accuracy of NT-proBNP alone (AUC 0.92, 95% CI 0.90–0.94, p for comparison = 0.64, Fig. 4A). BMP10 did not outperform NT-proBNP among patients with eGFR < 60 ml/min/1.73 m2 (Supplemental Fig. 1).
Fig. 4
Receiver operating characteristic curves comparison of BMP10 with high-sensitivity cardiac troponin T (hs-cTnT), N-terminal pro-B-type natriuretic peptide (NT-proBNP), and the combination of BMP10 and NT-proBNP for the diagnosis of acute heart failure in all patients (n = 933, Fig. 3A), patients with a history of atrial fibrillation (n = 284, Fig. 3B)
Subgroup analysis: atrial fibrillationSubgroup analysis in patients with a history of atrial fibrillation (n = 284) revealed a reduction in the diagnostic accuracy of all three biomarkers (Fig. 4B). AUC for BMP10 was 0.78 (95% CI 0.69–0.86), AUC for NT-proBNP was 0.75 (95% CI 0.66–0.84, p for comparison = 0.69), and AUC for hs-cTnT was 0.61 (95% CI 0.51–0.70, p for comparison < 0.05). Combining BMP10 and NT-proBNP did not improve the diagnostic accuracy as compared to NT-proBNP alone (AUC 0.78, 95% CI 0.70–0.87, p for comparison = 0.58).
Characterization of plasma BMP10 by its correlation with established blood biomarkersCorrelation between different blood biomarkers is depicted in Fig. 5. Plasma BMP10 concentration showed a strong correlation between NT-proBNP (0.71, p < 0.001) and MR-proADM (0.63, p < 0.001).
Fig. 5
Spearmen’s correlation coefficients between different blood biomarkers. Bio-ADM bioactive adrenomedullin, BMP10 Bone Morphogenetic Protein 10, CKMB creatinine kinase isoenzyme-MB, CRP C-reactive protein, eGFR estimated glomerular filtration rate, Hb hemoglobin, hs-cTnT high-sensitivity cardiac troponin T, IL-6 interleukin-6, MR-proADM mid-regional proadrenomedullin, NS not significant, NT-proBNP N-terminal pro-B-type natriuretic peptide, PCT procalcitonin
Plasma BMP10 and cardiac morphology and functionThere was a weak correlation between plasma BMP10 level and parameters of cardiac morphology and function, particularly left atrial size (Supplemental Table 2).
BMP10 and AHF triggersBMP10 concentration differed according to the trigger of AHF, with the highest values observed in AHF triggered by tachyarrhythmia 3.88 (2.84–4.72) ng/mL (Fig. 6).
Fig. 6
Plasma BMP10 concentration among patients with different triggers of AHF. Plasma BMP10 concentrations among patients with different triggers of AHF: arrhythmia 3.88 (2.84–4.72) ng/mL, infection 3.21 (2.43–4.19) ng/mL, and ischemia 2.49 (2.09–3.39) ng/mL. AHF acute heart failure, BMP10 Bone Morphogenetic Protein 10
We further tested the ability of BMP10, NT-proBNP, and hs-cTnT to identify AHF cases triggered by specific triggers.
ArrhythmiaAUC for BMP10 to identify arrhythmia-triggered AHF profile from the entire acute dyspnea cohort was the highest (0.78, 95% CI 0.75–0.82), followed by NT-proBNP (AUC 0.73, 95% CI 0.69–0.76, p for comparison 0.021) and hs-cTnT (0.56, 95% CI 0.52–0.61, p for comparison < 0.001; Supplemental Fig. 2A).
Myocardial ischemiaHs-cTnT performed best for myocardial ischemia-related AHF (AUC 0.85, 95% CI 0.80–0.90), followed by NT-proBNP (0.71, 95% CI 0.65–0.77), and BMP10 (0.57, 95% CI 0.50–0.63). The combination of BMP10 and NT-proBNP did not outperform NT-proBNP alone (AUC 0.69, 95% CI 0.63–0.75, p for comparison = 0.556, Supplemental Fig. 2B).
InfectionFor infection, the AUCs were as follow: 0.77, 95% CI 0.73–0.81 for NT-proBNP, 0.68, 95% CI 0.64–0.73 for BMP10, and 0.67, 95% CI 0.62–0.71 for hs-cTnT. The combination of BMP10 and NT-proBNP again did not outperform NT-proBNP alone (AUC 0.76, 95% CI 0.72–0.80, p for comparison = 0.766, Supplemental Fig. 2C).
Prognostic implicationsThe prognostic properties of BMP10 were investigated in 933 acute dyspnea patients and in a subgroup of 502 patients with adjudicated AHF. Within the acute dyspnea cohort, 29% (267 out of 933) of the patients died within the 720-day follow-up period (Supplemental Table 3). Among the AHF patients, the mortality rate was even higher, with 38% (188 out of 502) of the patients dying within the 720-day follow-up period (Supplemental Table 4).
Prognostic role of BMP10 in acute dyspneaPlasma BMP10 concentration was a strong predictor of mortality in patients with acute dyspnea, with patients in the fourth quartile having nearly four-times the mortality of patients in the first quartile (Fig. 7A). As a continuous variable in univariable analysis, the HR was 1.22 (95% CI 1.17–1.28, p < 0.001). However, after multivariable adjustment including NT-proBNP, BMP10 lost its predictive value (HR 1.01, 95% CI 0.94–1.09), p = 0.745, (Supplemental Table 5).
Fig. 7
Hazard curves of mortality in the overall group of patients with acute dyspnea (A) and the subgroup of acute heart failure (B) stratified by quartiles of plasma BMP10 levels at presentation. In the subgroup of acute heart failure, also the composite of mortality or rehospitalization for acute heart failure (C) is shown. BMP10 Bone Morphogenetic Protein 10, Q quartile
Prognostic role of BMP10 in AHFPlasma BMP10 concentration was a strong predictor of mortality in patients with adjudicated AHF, with patients in the fourth quartile having about three times the mortality of patients in the first quartile (Fig. 7B). As a continuous variable in univariable analysis, the HR was 1.16 (95% CI 1.09–1.23, p < 0.001). However, after multivariable adjustment, BMP10 lost its predictive value (HR 1.02, 95% CI 0.94–1.10, p = 0.711). Similar findings were found for the composite of death or AHF rehospitalization.
The fraction of new informationThe added value of BMP10 for predicting the risk of death in acute dyspnea, death in AHF, and death or rehospitalization for AHF was 0.2%, 0.2%, and 2%, respectively. The risk was estimated for a follow-up time of 720 days.
留言 (0)