
記住我
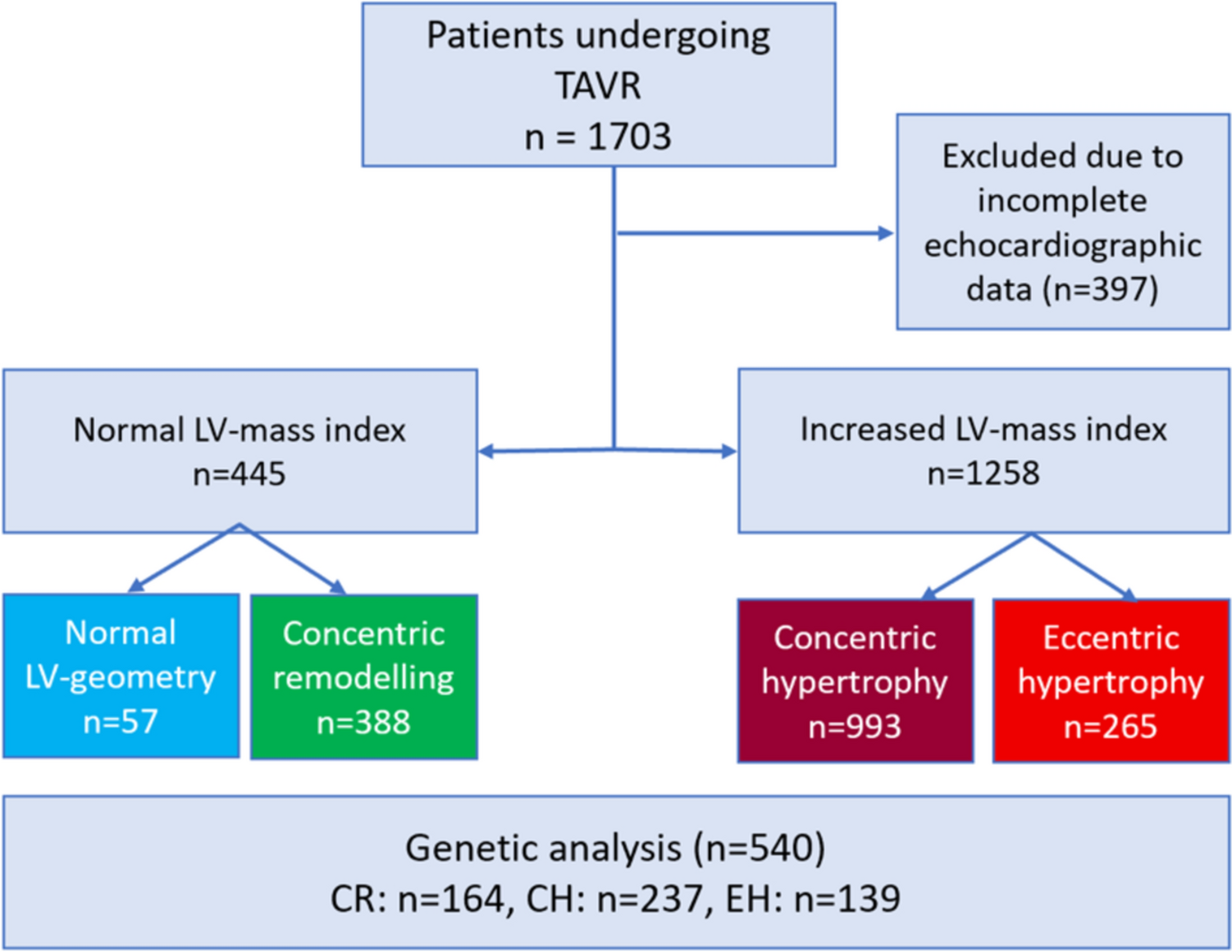
Between January 2015 and December 2022, 1703 patients underwent TAVR, received sufficient pre-TAVR echocardiography, and were included in the analysis. The mean age was 80 ± 6 years (range 35–97 years). Of these patients, 829 were male (49%). The patient cohort was divided into four groups according to their pre-TAVR hypertrophy pattern as described in the methods: NG was found in 57 patients (3.3%), CR in 388 patients (22.8%), CH in 993 patients (58.3%), and EH in 265 patients (15.6%).
Patients with EH had the highest logistic EuroSCORE I and II, and statistically significant differences were found between the groups CR versus CH and CR versus EH regarding EuroSCORE I and EuroSCORE II (p = 0.001). Compared to the other groups, more patients in the EH group were in NYHA-class III or IV and had a higher rate of left bundle branch blocks. The CH group had the highest proportion of women (61%). Statistically significant differences between the groups were found for logistic EuroSCORE I, II, higher NYHA classification, nicotine abuse, gender distribution, age, impaired renal function (GFR < 60 ml/min), previous myocardial infarction, and peripheral artery disease (Table 1). In a subgroup analysis of 527 patients, 8 (1.3%) additionally received a MitraClip in cases of severe mitral valve insufficiency prior to TAVI. There was no difference between the groups regarding the MitraClip rate. In a further subgroup analysis of 70 patients who underwent cardiac MRI, 5 (7.1%) showed pathological T1 relaxation times, suggesting possible cardiac amyloidosis. Regarding measured echocardiographic parameters, the highest mean aortic gradient was found in patients with CH, while the highest ejection fraction was measured in patients with CR. Patients with EH had the lowest preprocedural ejection fraction (43.2 ± 12.4%, p = 0.001), a low mean aortic gradient, and were associated with a high rate of higher-grade concomitant valve pathologies. Statistically significant differences between the groups were observed for ejection fraction and higher-grade aortic, mitral, and tricuspid valve insufficiency (Table 1, for all group comparisons via post hoc test, see the Supplementary Table).
Table 1 Baseline characteristics of the patients that were included into this studyProcedural characteristics and postprocedural outcomeMost valves were implanted using the transfemoral approach. The most frequent implanted valves were the Edwards Sapien (57.4%) and the Medtronic CoreValve (41.1%). Self-expanding valves (SEV) were most frequent in the CH group (43%), while balloon expending valves (BEV) were mostly applied in patients with EH (74%) followed by CR (68%) and NG (67%). There were significantly more SEV in the CH group compared to EH (p < 0.001) and CR (p = 0.002). The average annulus size was 26.8 ± 3.0 mm. The overall 30-day all-cause mortality was 3.7%, with the highest proportion (n = 3, 5.3%) in the NG group (Fig. 2). 26 patients (1.6%) suffered from peri- or postoperative strokes: 1 patient in group NG (1.7%), 7 patients in group CR (1.8%), 14 patients in group CH (1.4%), and 4 patients in group EH (1.5%). 49 cases (3.0%) of major or life-threatening bleedings according to the VARC-2 criteria occurred. Within the first 72 h after TAVR, a myocardial infarction according to VARC-2 occurred in 6 patients (0.4%). Overall, 156 new pacemakers (9.5%) had to be implanted after the TAVR (NG 8.8%, CR 8.2%, CH 9.2% and EH 10.6%, respectively). The rate of new pacemakers after TAVR was 10.0% for SEV and 8.2% for BEV (p = 0.092).
Fig. 2
Kaplan–Meier estimates of the 30-day survival function after TAVR in the 4 groups determined by hypertrophy. Blue: patients with normal hypertrophy, green: patients with concentric remodeling, red: patients with concentric hypertrophy, orange: patients with eccentric hypertrophy
One-year and mid-term outcomeFollow-up data for the patient cohort were collected up to seven years after TAVR. 397 patients were excluded due to missing data. A statistically significant difference between the groups regarding the postprocedural outcome was calculated for all-cause mortality after 30 days, 1 year and 4 years (p = 0.001 for 30 days, 1 year and 4 years) (Figs. 2 and 3). The overall mortality for SEV was significantly higher (38.1%) compared to BEV (20.7%, p < 0.001). Furthermore, the overall mortality was not significantly higher in patients with smaller annulus size (small annulus 35.9% versus 30.1%, p = 0.229).
Fig. 3
Mid-term survival after TAVR; Kaplan–Meier estimates of the survival function after TAVR in the 4 groups determined by hypertrophy. Blue: patients with normal hypertrophy, green: patients with concentric remodeling, red: patients with concentric hypertrophy, orange: patients with eccentric hypertrophy
At the 30 day timepoint, a statistical difference was found between the NG and CR groups, while no difference in survival between the CH and EH group was observable. The overall 1-year all-cause mortality rate was 14.2%. The EH group had the worst outcome in comparison the other groups (p < 0.001). Mid-term survival up to 4 years is illustrated in Fig. 3. Survival rates after 4 years were 73.6% (NG), 71.9% (CR), 73.1% (CH) and 58.1% (EH). The estimated survival functions are split according to the hypertrophy pattern groups.
Multivariate analysisA multivariate Cox regression was performed based on the significant results in the previously performed univariate regression. An association between all-cause mortality and age (odds ratio (OR): 1.030) as well as atrial fibrillation (OR: 1.576) was observed (p < 0.001). Moreover, preserved ejection fraction was associated with higher survival rates (OR: 0.973, p < 0.001, Table 2).
Table 2 Multivariate analysis of the significant influencing factors observed in the univariate regressionGenetic analysisA subgroup of 540 AS cases with three distinct hypertrophic patterns (CR, CH, EH) were included in the genetic analysis (80.7 ± 6.2 years of age). 43.9% (n = 237) of patients displayed CH, while 25.7% (n = 139) demonstrated EH and 30.4% (n = 164) CR phenotypes. There was no statistically significant difference between the occurrence of CAD and arterial hypertension in these groups, which can be considered also causative for the EH or CH phenotype, respectively (Table 3). The percentile values of the polygenic risk scores (PRS) differed significantly in group comparisons. Particularly, the mean percentile values of hypertrophic cardiomyopathy polygenic risk scores (HCM-PRS) were considerably higher in the CH group when compared to the EH group (Mean percentiles ± standard deviation: CH = 49.5 ± 30.1, EH = 40.3 ± 29.3, p = 0.011). For all three hypertrophy categories, a negative Pearson correlation of the DCM-PRS and the HCM-PRS percentiles was observed, which was significantly different from zero. CR showed a weak inverse correlation of the DCM- and the HCM-PRS percentiles, which was—0.30 [− 0.44, − 0.16], p < 0.001, whereas EH and CH showed a moderate correlation of − 0.51 [− 0.63, − 0.38], p < 0.001 and − 0.47 [− 0.57, − 0.37], p < 0.001 (Fig. 4). This correlation has been described before [28] and could be reproduced in our cohort.
Table 3 Baseline characteristics of the genetic cohortFig. 4
Scatterplot depicting the distribution of the measured PRS for DCM and HCM. There was an inverse correlation between the two measured polygenic risk scores in all three groups. Overall in patients with a high HCM-PRS value, low values for the DCM-PRS were observed. CH concentric hypertrophy (purple), CR concentric remodeling (green), EH eccentric remodeling (orange), DCM-PRS polygenic risk score for dilated cardiomyopathy, HCM-PRS polygenic risk score for hypertrophic cardiomyopathy
In a second step, cardiovascular risk factors, such as sex, arterial hypertension, renal insufficiency and dyslipidemia, were considered using two multiple logistic regression models for modeling the occurrence of a EH and CH with reference to CR. Concerning the prediction of hypertrophy EH versus CR, we can state that HCM-PRS had a significant influence (p = 0.046). There was an inverse correlation between the elevated HCM-PRS percentiles and the occurrence risk of EH (regression coefficient: − 0.011). However, the same difference in percentiles had no significant influence for CH compared to CR (p = 0.863). Moreover, no other PRS had a significant influence in none of the two models (Table 4).
Table 4 PRS values for the CH and EH subgroup
留言 (0)