Lp(a) is considered an independent risk factor for the occurrence of cardiovascular diseases such as coronary artery disease (CAD), arteriosclerosis (AS), and myocardial infarction [1, 5, 16]. Nevertheless, its significance, especially in elderly patients, is sometimes controversially discussed in the literature [17,18,19,20].
Our study is the first to show no effect of Lp(a) on aortic valve calcification and prognosis in a general population of patients with severe AS undergoing TAVR. Our main findings are as follows: first, elevated Lp(a) levels showed no impact on the degree of aortic valve calcification in the studied TAVR cohort. Second, these results were also reflected in the subgroup analysis of male and female patients. Third, an elevated Lp(a) value ≥ 60 mg/dl demonstrated no prognostic influence on all-cause mortality at 30 days and 3 years post-TAVR. These results provide an essential addition to existing knowledge and raise questions about the role of Lp(a) in aortic valve calcification.
Study cohort
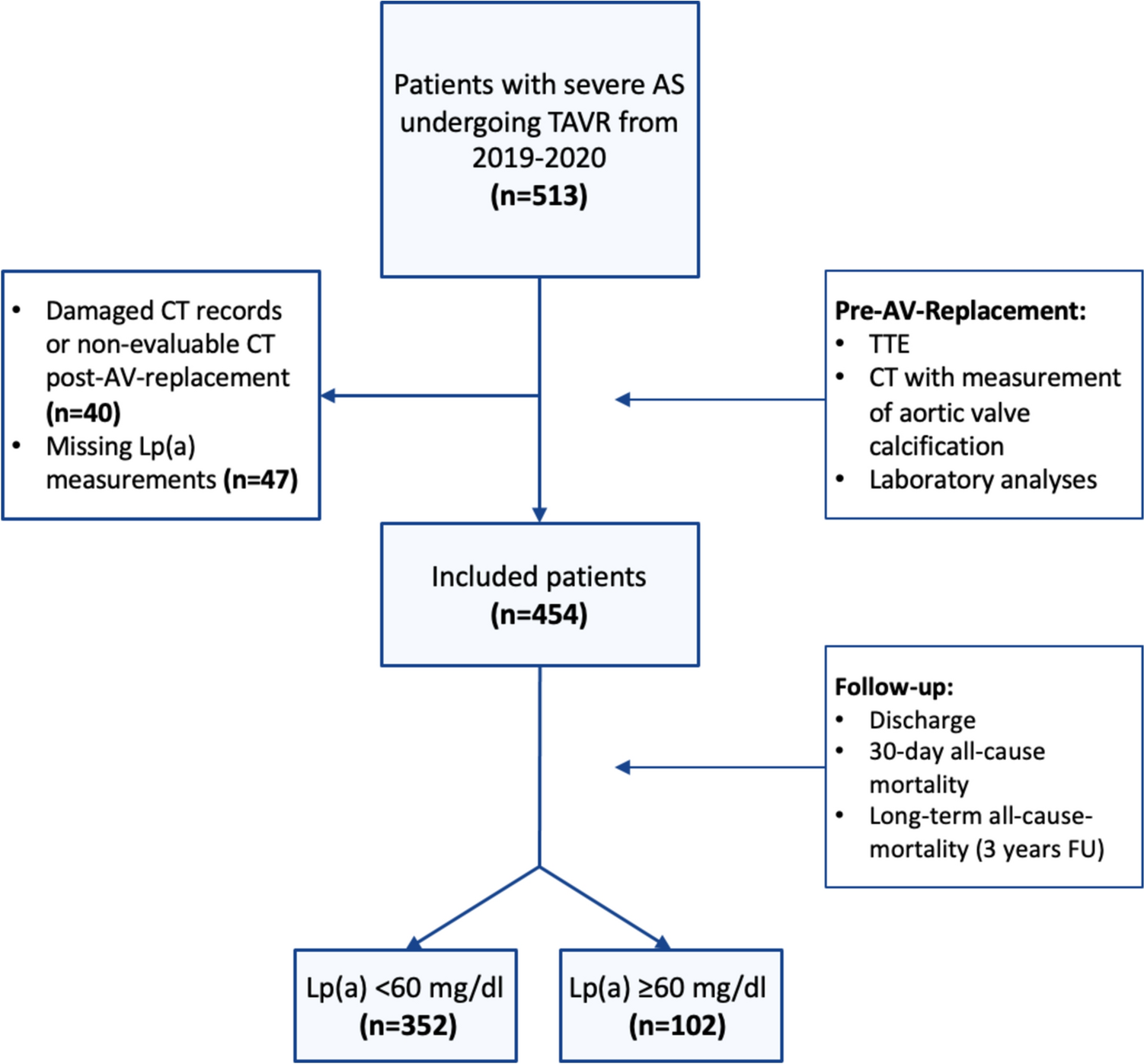
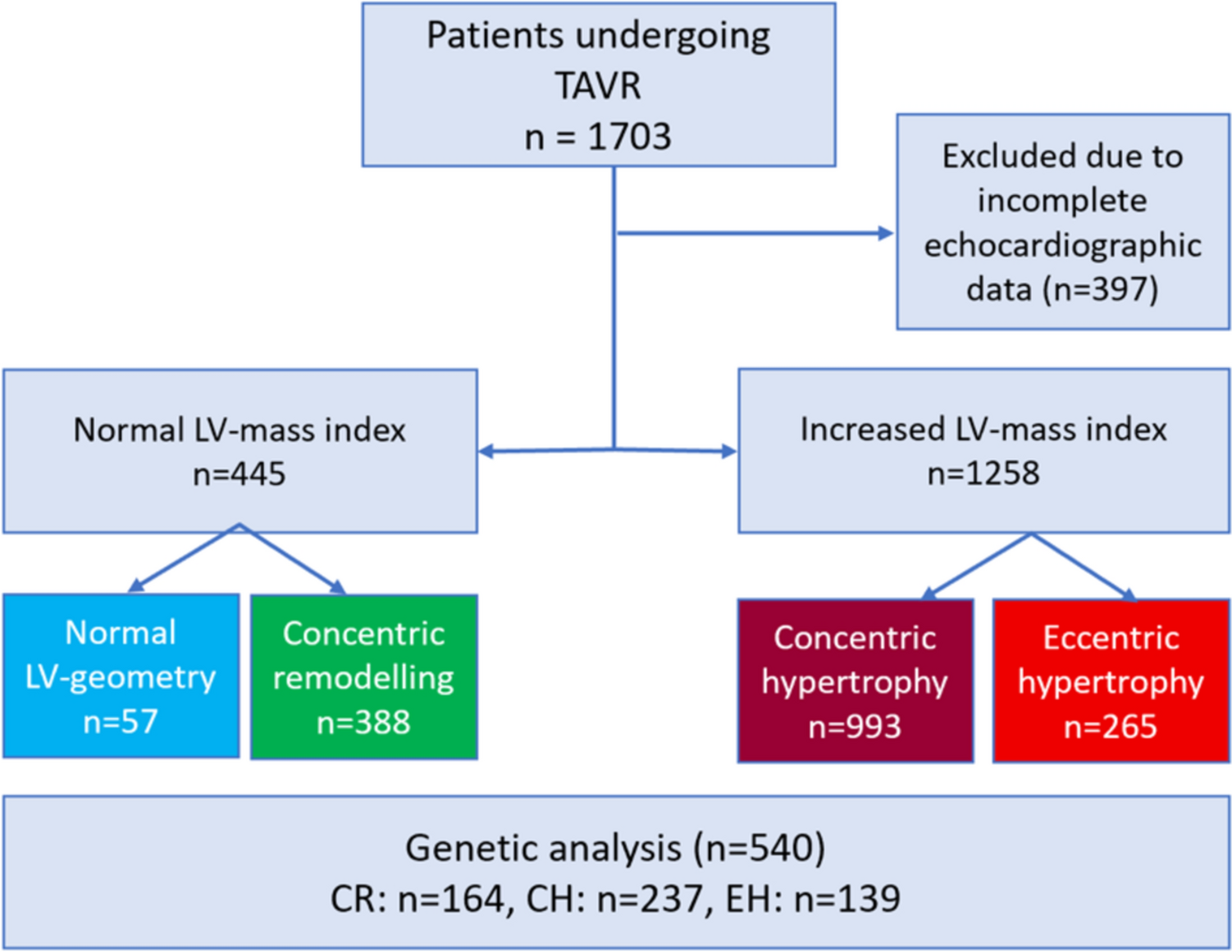
The study cohort of 454 patients comprised multimorbid TAVR patients regarding baseline data and preexisting conditions. Consistent with the findings of Mauri et al. (15,344 patients from five German TAVR centers), the patients exhibited a similarly high age (average 81 years) and a pronounced cardiovascular risk profile [21]. The echocardiographic parameters obtained, with a ΔPm of 44.15 ± 15.72 mmHg and an AVA of 0.75 ± 0.20 cm2, align with other TAVR and SVAR registries [22, 23]. The restriction of the valve opening area is attributed to complex fibrotic and calcific remodeling [9, 24]. Consequently, it is not surprising that this study also demonstrated a correlation between severe aortic valve calcification and higher Vmax and delta Pm. Furthermore, our finding indicating an association between male gender and higher levels of calcification are consistent with the ECS/EACTs guidelines cut-off values for men with calcified aortic stenosis, which specify higher Agatston thresholds for men in native CT scans [9]. The method used in this study to evaluate the contrast-enhanced CT images with the 3Mensio™ software was also employed in the TAVR registry by Kim et al. [25] Initial studies have indicated that the results of calcification evaluation using 3Mensio are potentially comparable to those obtained with other software, such as CVI 42™ (Circle Cardiovascular Imaging Inc., Canada) or SyngoVia™ (Siemens Healthcare GmbH, Germany) [26]. Nevertheless, the lack of standardized protocols for contrast-enhanced CT images may continue to hinder comparability [25].
Lp(a) as cardiovascular risk factor in aortic stenosis
The prognostic utility of Lp(a) in advanced stages of AS is not well established, and there are currently no standardized cut-off levels for Lp(a) [12, 13]. Different guidelines and consensus statements suggest varying cut-offs for elevated Lp(a), ranging from 30 to 90 mg/dL [27]. However, lipid apheresis guidelines specify a 60 mg/dL cut-off [1, 14]. Given that lipid apheresis is presently the only therapeutic option for reducing Lp(a) levels, we adopted this cut-off in our study. In general, Lp(a) levels vary widely, from almost 0 to > 200 mg/dl, [28] with values as low as approximately 20 mg/dl associated with a steadily increasing risk of cardiovascular diseases such as myocardial infarction, stroke, or aortic valve stenosis. [29,30,31] Additionally, there is a 2- to fourfold median difference in plasma Lp(a) levels among different ethnic groups [27], with about 20% of the Caucasian population having Lp(a) levels > 50 mg/dl [32], a prevalence that is higher in African ethnic groups and lower in Asian ethnic groups [33, 34]. The Lp(a) distribution in this study resembles previously described distributions [35, 36], but there is a higher proportion of participants with values ≥ 50 mg/dl (26.0%), matching the Lp(a) distributions observed in patient groups with a high cardiovascular burden [36].
Elevated Lp(a) levels are associated with an increased risk of cardiovascular disease (CVD) and a higher severity of coronary artery disease (CAD) [1, 37]. In patients with CAD, those with elevated Lp(a) levels above 150 nmol/l were more likely to have severe CAD that is more difficult to treat [38]. However, in this older and multimorbid TAVR cohort, no differences were found in the proportion of patients with CAD between the groups with an Lp(a) cut-off of 60 mg/dl, whereas the proportion of patients with CAD is in the upper range compared to other TAVR registries [21, 39]. These results corroborate the assertion by Cicec et al. that Lp(a) exerts a role as a risk factor for CAD primarily in younger patients (aged < 65 years) and appears to lose significance with age [17]. Conversely, studies have demonstrated that elevated Lp(a) levels remain an independent risk factor for coronary heart disease in slightly older patients with a median age of 71 years. [35] Nevertheless, the clinical benefit of a reduction in elevated Lp(a) remains unclear in these studies [35, 40]. This is of particular interest in regard to the fact that several phase III trials for a specific drug-based reduction of Lp(a) are already underway [10, 11].
There is limited evidence on the direct or quantitative impact of Lp(a) on aortic valve calcification (AVC) [41]. Our analysis shows that despite the known association of Lp(a) with various cardiovascular diseases, no significant influence on AVC in elderly patients with preexistent severe AS could be observed. Lp(a)’s influence might be restricted to the early stages of calcification (initiation phase), losing significance as calcification progresses [41]. In the younger patients (mean age 58 years) from the ASTRONOMER trial with mild to moderate stenosis and elevated Lp(a), a faster disease progression with Vmax increase could be described [5]. This finding is consistent with the results reported by Vongpromek et al. [42]. Whereas a faster progression of ΔPm and Vpeak in patients with higher Lp(a) values were not significant in the PROGRESSA [43] and SALTIRE2 [44] trial [45]. It is conceivable that the impact of Lp(a) in AS is limited to the younger patients with AVC, who are more likely to be included in SAVR cohorts [46]. In a smaller cohort of 210 patients, Farina et al. [47] demonstrated that bioprosthetic valves (70% SVAR) exhibited faster degeneration in the presence of elevated Lp(a) levels. However, it remains unclear whether this finding can be extrapolated to the typically older TAVR patient population.
Prognostic value of Lp(a) in TAVR
In the highly debated field regarding the influence of Lp(a) in multimorbid, elderly patients with advanced severe aortic stenosis, this study found no evidence of a prognostic impact on all-cause mortality. Our results showed no significant differences in 30-day or long-term all-cause mortality, with a mean follow-up time of 38 months. Similar to this study, there are 30-day mortality rates of 2.1% in other German TAVR registries [21]. However, there are no other existing analyses on the impact of Lp(a) on mortality rates in TAVR patients. The observation that both groups exhibit a similarly high risk may be influenced by the bias that Lp(a) is recognized as a cardiovascular risk factor, prompting these patients to attend regular follow-ups with their cardiologists. However, it should also be noted that most TAVR patients are routinely subjected to close, structured follow-up care after the procedure, irrespective of their Lp(a) levels.
Furthermore, no significant differences were observed in the echocardiographic parameters at discharge, including ΔPmean, ΔPpeak, and the prevalence of PVL, between patients with elevated Lp(a) levels (> 60 mg/dl) and those with lower Lp(a) levels. The extent and distribution of calcification are recognized as factors influencing PVL post-TAVI [48]. Since Lp(a) did not show any impact on calcification in CT imaging in our study, this may partly explain the lack of differences in PVL prevalence between the groups.
Limitations
This study has several limitations. First, it is a retrospective observational study with only 454 patients, which means that potential biases leading to overestimation or underestimation of effects cannot be excluded. Second, patients from a single center and a very specific multimorbid patient cohort were included, which might limit the generalizability of the results to other populations due to possible additional factors not explicitly captured here. However, despite being a single-center cohort, the study population demonstrates good comparability with other larger multicenter TAVR registries [21].
Additionally, the lack of uniform thresholds and measurement methods for Lp(a) and the absence of standardized procedures for assessing aortic valve calcification in contrast-enhanced CT scans further restrict the generalizability of the findings.

留言 (0)