
記住我
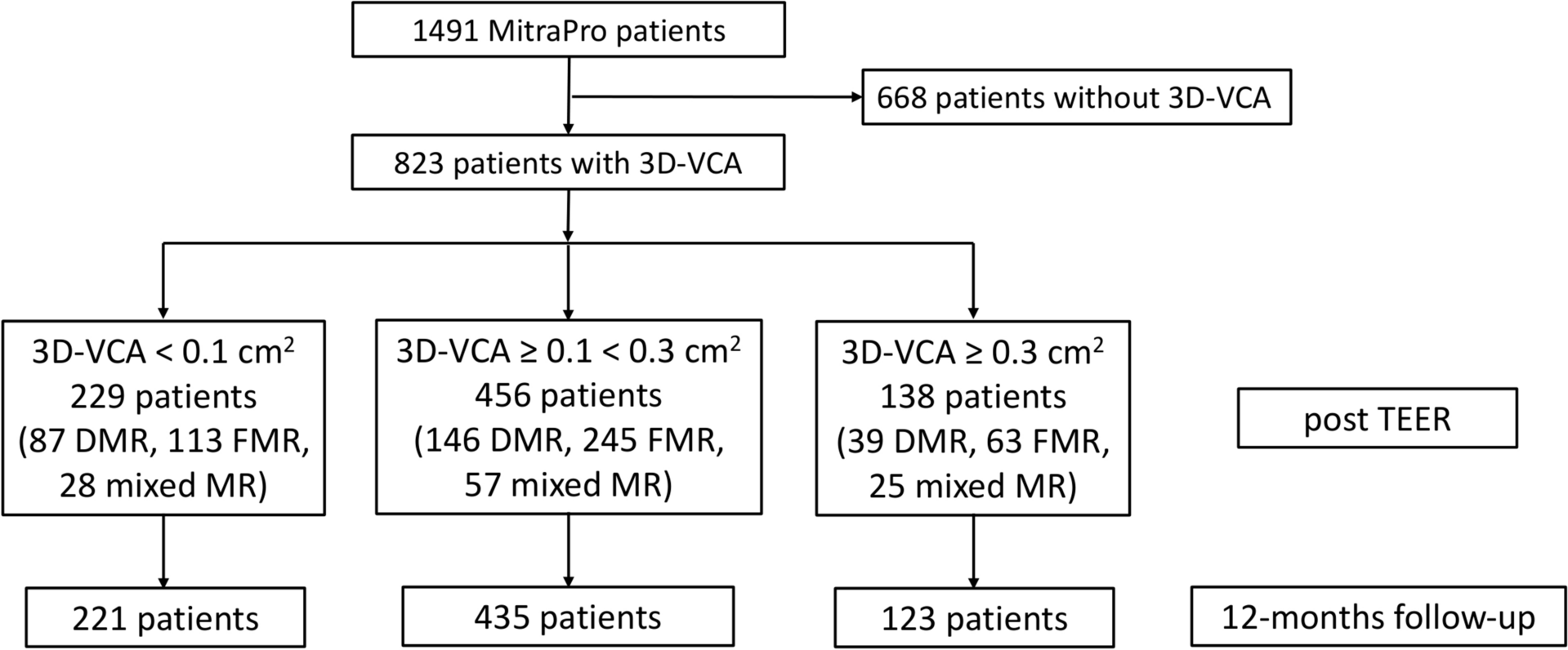
The MITRA-PRO registry enrolled 1491 consecutive individuals with primary, secondary, or mixed MR who underwent mitral TEER and intraprocedural echocardiographic assessment of residual MR. In a real-world scenario, in 823 patients 3D-VCA before and after mitral TEER were part of the MitraScore calculations (Fig. 1). Following a ROC analysis at a 3D-VCA of 0.07 cm2, mortality significantly increased (1-year mortality for 3D-VCA post-mitral TEER ≥ 0.07 cm2: 16.5% vs. < 0.07 cm2: 7.8%; p = 0.005), highlighting a 3D-VCA value of rounded 0.1 cm2 as a relevant cutoff for survival assessment. Furthermore, a 3D-VCA of 0.27 cm2 was previously described as moderate residual MR (3). Therefore, we allocated the patients to 3 groups: 229 (27.8%) with a 3D-VCA of < 0.1 cm2, 456 (55.4%) with a 3D-VCA ≥ 0.1 < 0.3 cm2, and 138 (16.8%) with a 3D-VCA of ≥ 0.3 cm2. Group assignment was based on the 3D-VCA measurement post-mitral TEER.
Baseline and procedural characteristicsThe baseline characteristics of the 3D-VCA groups are shown in Table 1 and were similar, except a higher systolic pulmonary artery pressure (sPAP) in the 3D-VCA ≥ 0.3 cm2 group. Furthermore, a greater number of TEER devices were used, and the procedure time was significantly longer in patients with a 3D-VCA ≥ 0.3 cm2 post-mitral TEER (supplementary Table 2). Both CVP and LAP were elevated before and after mitral TEER in the 3D-VCA ≥ 0.3 cm2 group compared to the 3D-VCA < 0.1 cm2 or 3D-VCA ≥ 0.1 < 0.3 cm2 groups (supplementary Table 2).
Table 1 Patients characteristics at baselinePeri-interventional complications and in-hospital outcomesPeri-interventional complications were rare across all groups, with no significant differences observed, as detailed in supplementary Table 2. During the hospital stay following the index procedure, there were 3 deaths in the 3D-VCA < 0.1 cm2 group, 9 deaths in the 3D-VCA ≥ 0.1 < 0.3 cm2 group, and 4 deaths in the 3D-VCA ≥ 0.3 cm2 group, resulting in in-hospital mortality rates of 1.3%, 2.0%, and 2.9%, respectively (p = 0.56; supplementary Table 2). Additionally, the rates of in-hospital major adverse cardiovascular events (MACE) and major adverse cardiovascular and cerebrovascular events (MACCE) were similar across all groups (supplementary Table 2).
Predictors of 3D-VCA ≥ 0.3 cm2To identify predictors of residual MR a multivariate analysis was performed. It revealed sPAP (per 20 mmHg), severe baseline MR and permanent AF as independent predictors of a 3D-VCA ≥ 0.3 cm2 (Table 2).
Table 2 Multivariable predictors of 3D VCA ≥ 0.3 cm2 after TEER at baseline1-year mortality according to 3D-VCA1-year clinical follow-up was completed in 779 patients (94.7%) of the total cohort (3D-VCA < 0.1 cm2: 221 patients, 96.5%; 3D-VCA ≥ 0.1 < 0.3 cm2: 435 patients, 95.4%; 3D-VCA ≥ 0.3 cm2: 123 patients, 89.1%). Notably, patients with trace or mild residual MR showed significantly lower 1-year mortality rates. Specifically, the 1-year mortality rates were 10.5% in the 3D-VCA < 0.1 cm2 group, 16.0% in the 3D-VCA ≥ 0.1 < 0.3 cm2 group, and 24.8% in the 3D-VCA ≥ 0.3 cm2 group (Fig. 2). A higher 3D-VCA measurement post-mitral TEER was associated with increased 1-year mortality, as shown in Fig. 3.
Fig. 3
Association of 3D-VCA and 1-year mortality. 3D-VCA assessing residual MR following transcatheter mitral valve repair (TEER) related to 1-year mortality. Bar graphs indicate grouped 3D-VCA post TEER (< 0.1 cm2, ≥ 0.1 < 0.3 cm2 and ≥ 0.3 cm2). OR odds ratio
An analysis with the 3 predefined 3D-VCA groups revealed that group ≥ 0.1 < 0.3 cm2 is significantly different from the 3D-VCA < 0.1 group (p = 0.01) and 3D-VCA ≥ 0.3 group (p < 0.001) demonstrating increasing 1-year mortality over these groups (Fig. 3). Furthermore, re-intervention or mitral valve surgery was more frequently required in the 3D-VCA ≥ 0.3 cm2 group (3D-VCA < 0.1 cm2: 1.1%; 3D-VCA ≥ 0.1 < 0.3 cm2: 4.4%; and 3D-VCA ≥ 0.3 cm2: 8.8%; p = 0.016).
Comparison of 3D-VCA to LAP and 2D-TOEPatients were categorized based on MR severity: MR 0/I (none, trace, mild MR), MR II (moderate MR), or MR III (severe MR), as determined by post-procedural TOE following mitral TEER. We observed a 1-year mortality rate of 15.9% for MR 0/I, 22.4% for MR II, and 25.0% for MR III, as assessed by post-procedural 2D-TOE, indicating a trend without a significant difference (log-rank p-value: 0.063). Similarly, we conducted an analysis based on LAP post-TEER, categorizing patients into LAP < 20 mmHg, LAP 20–35 mmHg, and LAP > 35 mmHg. The 1-year mortality rates were 16.2% for LAP < 20 mmHg, 16.3% for LAP 20–35 mmHg, and 25.0% for LAP > 35 mmHg, again showing a trend without a significant difference (log-rank p-value: 0.064). A c-statistic for predicting 1-year mortality was performed: 3D-VCA: 0.6 (CI: 0.52–0.63), 2D-TOE: 0.5 (CI: 0.43–0.58) and LAP:0.5 (CI: 0.43–0.56).
Interobserver variabilityTo estimate interobserver variability corelab 3D-VCA data of 47 patients were compared to the corresponding 3D-VCA assessed by the investigators. Pearson correlation coefficient (PCC) and Bland Altman Analysis of 3D-VCA (investigator versus corelab) demonstrated good reliability (PCC: 0.86; p < 0.001; supp. Figure 1).
12-months clinical and echocardiographic follow-upIn the MITRA-PRO cohort, mitral TEER reduced 3D-VCA significantly compared to baseline. In transthoracic echocardiography, MR grading improved at discharge compared to baseline across all groups, with significantly better results in patients with a 3D-VCA < 0.1 cm2 (Supplemental Table 3). However, at 12-month follow-up, the number of patients who underwent transthoracic echocardiography at individual study centers was low (3D-VCA < 0.1 cm2: 38; 3D-VCA ≥ 0.1 < 0.3 cm2: 83; 3D-VCA ≥ 0.3 cm2: 33), leading to no statistical difference in MR grading between the three 3D-VCA groups (supplemental Table 3).
Furthermore, NYHA classification was improved at 12-months follow-up after mitral TEER (Fig. 4A). Baseline NYHA classification was comparable in all 3D-VCA groups, while in 3D-VCA < 0.1 cm2 the number of patients with NYHA I/II at 12-months follow-up was significantly higher compared to 3D-VCA ≥ 0.3 cm2 indicating an association of residual MR and improvement of symptoms (Fig. 4A). Also, improvement in NYHA classification (at least one class) at 12-months follow-up following mitral TEER was significantly higher in 3D-VCA < 0.1 cm2 compared to 3D-VCA ≥ 0.3 cm2 (Fig. 4B), which further strengthens the hypothesis, that residual MR after mitral TEER is directly linked to symptomatic improvement.
Fig. 4
NYHA classification according to 3D-VCA groups. A Distribution of NYHA classification at baseline, discharge and 12-months follow-up according to 3D-VCA groups (< 0.1 cm2, ≥ 0.1 < 0.3 cm2 and ≥ 0.3 cm2). B NYHA improvement ≥ 1 class according to 3D-VCA groups (< 0.1 cm2, ≥ 0.1 < 0.3 cm2 and ≥ 0.3 cm2). 3D-VCA 3D-Vena Contracta Area
留言 (0)