
記住我
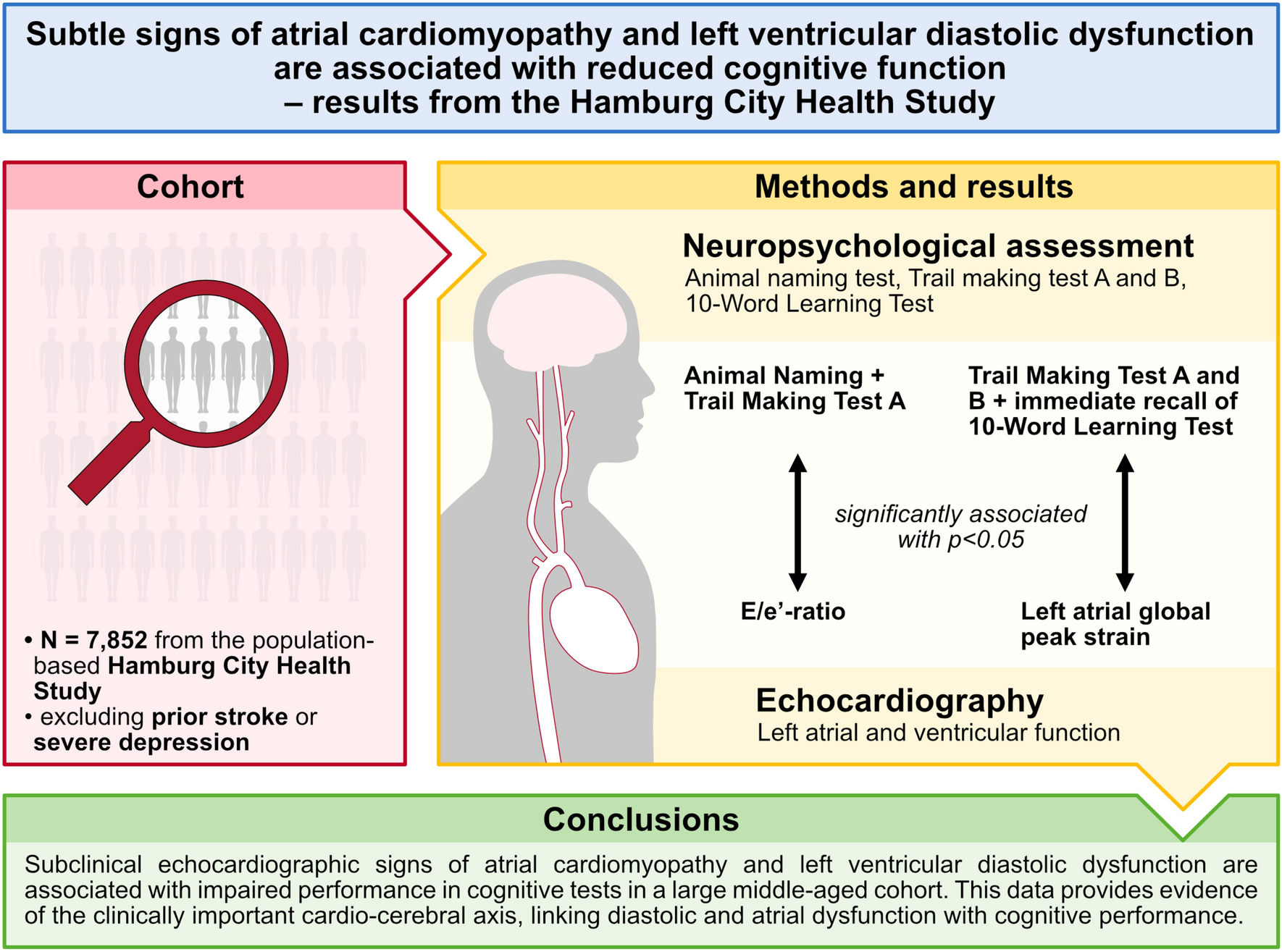
The HCHS enrolls inhabitants of Hamburg aged 45–74 years, identified by random sampling from the official inhabitant data file [17]. Data from the first 10,000 participants of the HCHS were available and selected for analysis. Of these, 8211 individuals received a transthoracic echocardiography examination. After exclusion of 359 individuals with prior/known stroke (N = 243) or severe depression (N = 116; defined as a score ≥ 15 in the Patient Health Questionnaire [18]), 7852 individuals were included in the final analyses for the present study.
Physical examinations were conducted by trained and certified medical staff according to standardized operation procedures and the data integrity was controlled by a detailed, predefined quality control algorithm [17]. Only quality-controlled data were used for statistical analyses in this study. A subgroup of 2069 participants with an increased risk for cerebrovascular diseases were invited to a cMRI examination.
The research protocol was approved by the local ethics committee of the Hamburg Chamber of Medical Practitioners (PV5131) as well as the Data Protection Commissioner of the University Medical Center of the University Hamburg-Eppendorf and the Data Protection Commissioner of the Free and Hanseatic City of Hamburg. The study has been registered at ClinicalTrial.gov (NCT03934957). All participants provided written informed consent.
Definition of clinical covariatesArterial hypertension was defined as systolic or diastolic blood pressure > 140 mmHg or > 90 mmHg, respectively, prescription of antihypertensive drugs or self-reported hypertension. Coding of diabetes mellitus was based on self-report, or a fasting plasma glucose ≥ 126 mg/dl or a non-fasting plasma glucose ≥ 200 mg/dl. Educational level was assessed according to the International Standard Classification of Education (ISCED) and divided into three groups: low (ISCED levels 0–2), medium (ISCED levels 3–4) and high (ISCED levels 5–8).
Transthoracic echocardiography examination acquisition and analysisSingle timepoint transthoracic echocardiography was systematically performed within the baseline examination program. The patients were examined in left lateral position with the Siemens Acuson SC2000 Prime ultrasound device (Siemens Healthineers, Erlangen, Germany). The examination followed a strictly standardized protocol, which included all established standard echocardiography views as well as Doppler velocimetry. Recordings were electrocardiogram-triggered and preferably performed with breath holding technique. For image analysis and quality assurance, standardized operating procedures were defined in agreement with the current guidelines of the American Society of Echocardiography and the European Association of Cardiovascular Imaging [19, 20]. Left ventricular ejection fraction (LVEF) was calculated from LV end-diastolic and end-systolic volumes using the modified Simpson’s rule [19]. The end-diastolic thickness of the interventricular septum was assessed in the parasternal long-axis view. Maximum and minimum LA volumes, and the LA ejection fraction (\(\frac}\text}}\) × 100) were calculated using the disk summation technique based on biplane measurements (apical four- and two-chamber view) [19]. If the LA volumes were only available from one plane, these values were used for analyses to avoid missing data. All volume-based measurements were indexed to body surface area.
The peak E-wave and peak A-wave velocities were recorded using pulsed wave Doppler with the sample volume placed between the mitral leaflet tips in the apical four-chamber view [20]. The peak e’-velocities were assessed using tissue Doppler imaging by placing the pulsed Doppler sample volume at the lateral (lateral e’) and septal (septal e’) regions of the mitral valve annulus in the apical four-chamber view [20]. The ratio of peak E-wave velocity and the average of peak e’-velocities (lateral and septal) was calculated as a non-invasive surrogate parameter of LV filling pressure (E/e’-ratio).
The global peak strain of the left atrium was measured by three different investigators using 2-D speckle tracking. The quality of each echocardiographic image and analysis was evaluated on a scale from 1 to 4 (1: no breathing, well-defined, correct angle; 2: no breathing, angle not quite optimal and/or more difficult to define; 3: respiration and/or very poorly defined but plausible curve; 4: heavy breathing and/or no legitimate curve). We excluded all participants who were rated as 4 due to insufficient image quality to perform strain analysis. After optimal positioning of the myocardial search region in the apical four-chamber view, the automatic contour detection process of the myocardium was started in real time (Fig. 1). However, in some cases, the endo- and epicardial detected frames did not cover the entire endocardium and epicardium in real time so that they had to be corrected manually. The QRS complex was used as the initiation of the strain calculation (R-R gating). The software Siemens syngo SC2000 Version 4.0 (Siemens Healthineers, Erlangen, Germany) was used to evaluate and quantify echocardiography data from certified investigators in a single reading center. All examiners were blinded to the subjects' clinical information.
Fig. 1
Exemplary measurement of left atrial global peak strain. Panel A: Apical 4-chamber view delineating the endocardial boundary of the left atrium in three sections (right wall, roof and left wall) as indicated by the respective colors. Panel B: Exemplary left atrial endocardial longitudinal strain curve derived from 2-D speckle-tracking. Panel C: Exemplary left atrial peak strain values for the three different sections and derived left atrial global peak strain value
Neuropsychological assessmentCognitive function was assessed using the Animal Naming Test (ANT), the Trail Making Test and a 10-Word Learning Test. The ANT is a semantic verbal fluency test in which the individuals are asked to list as many names of animals as possible within one minute. All responses are counted excluding repetitions and non-animal words. The Trail Making Test consists of two parts, which reflect different areas of the human cognitive function. During part A (TMT-A), the individuals are asked to connect all numbers from 1 to 25 on a paper in sequential order, testing the individual’s information processing speed. A successful completion of Part B (TMT-B) requires the connection of all dots from 1 to 13 and letters from A to L while alternating letters and numbers (as in 1-A-2-B-3-C…), assessing attention and executive function. In both cases, TMT-A and TMT-B, the time to completion of the test is recorded as the test result, with time limits of 180 s and 360 s for TMT-A and TMT-B, respectively. For the 10-Word Learning Test, ten non-associated words were read to the participants in a different order in three rounds. Then participants were asked to freely recall these ten words after each round gaining one point for every correct response, and the sum of correct answers from all three rounds was calculated (immediate recall, range 0–30). In addition, participants were again asked to reproduce the ten words after 5–10 min (delayed recall, range 0–10). This test assesses the memory function.
Cerebral magnetic resonance imagingA subgroup of participants with present cardiovascular risk factors underwent standardized cMRI using a 3-T Siemens Skyra MRI scanner (Siemens, Erlangen, Germany; N = 2069). Further details of the cerebral magnetic resonance imaging protocol in the HCHS have been described in previous publications [21]. In addition to signs of infarct residuals, WMH were segmented on T1-weighted and FLAIR images with FSL’s Brain Intensity Abnormality Classification Algorithm (BIANCA) [22] and Locally Adaptive Threshold Estimation (LOCATE) [23] as described in detail previously. WMH were further divided into periventricular (pWMH) and deep (dWMH) by a 10 mm distance threshold to the ventricles [24,25,26]. WMH load was calculated as the proportion of WMH to brain tissue volume (intracranial volume—ventricle volume) and logarithmized for further statistical analysis based on a right-skewed distribution. Logarithmic pWMH and dWMH load were calculated analogously.
Statistical analysisCategorical variables are given as absolute and relative frequencies, continuous variables as median (25th/75th percentile). We used multiple imputation to handle missing information on clinical covariates (information on missing values and imputations are provided in Supplementary Table 1). We performed linear regression analyses with incremental adjustment to examine the association of echocardiographic parameters with the performance on each of the neuropsychological tests. In a first step, we calculated age- and sex-adjusted regression analyses (model 1). In multi-variable-adjusted analyses, arterial hypertension, body mass index, total serum cholesterol concentration, diabetes mellitus, current smoking, AF, prior/known myocardial infarction, heart failure and educational level were added as additional covariates (model 2). In a third and final step, analyses were additionally adjusted for further echocardiographic parameters of the left ventricle (LVEF and end-diastolic thickness of the interventricular septum; model 3). In sensitivity analyses, we excluded individuals with known AF, heart failure, and prior myocardial infarction. A two-sided p-value ≤ 0.05 was considered statistically significant for all analyses. Analyses were performed with R v.4.0.3 (www.R-project.org).
留言 (0)