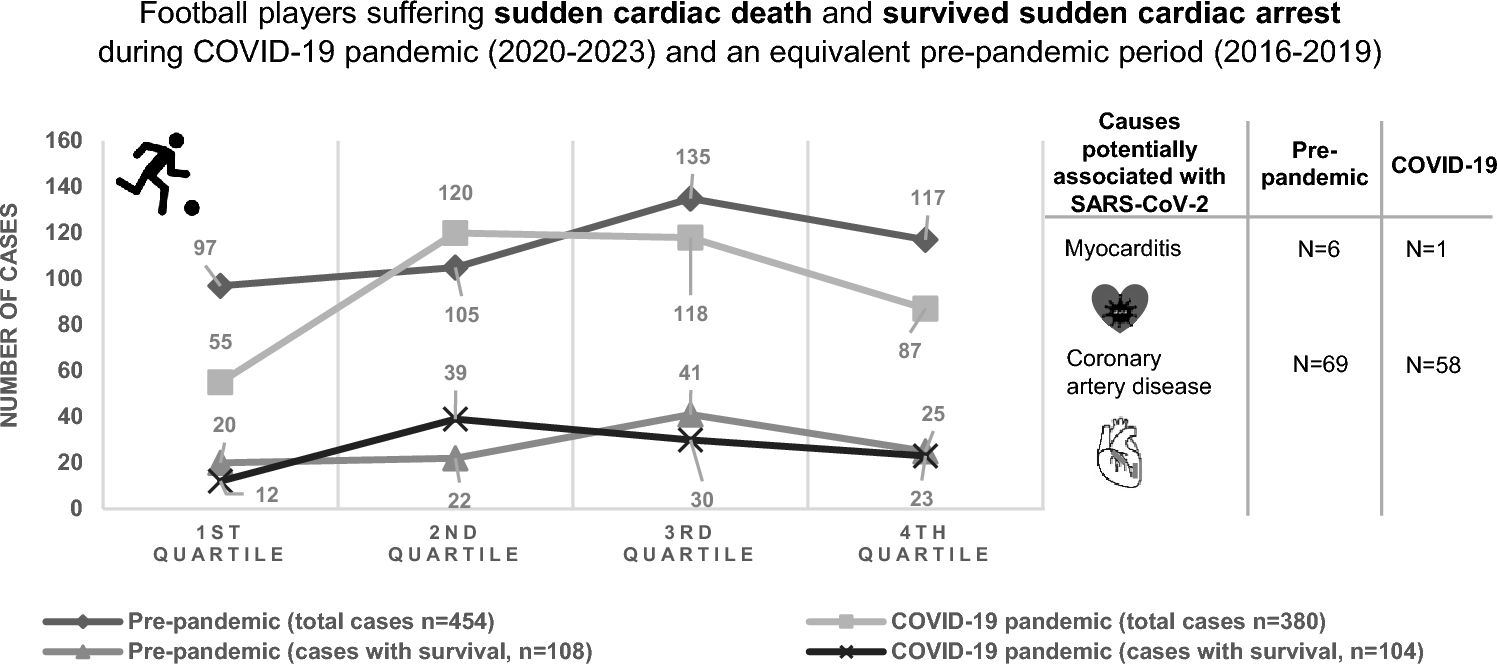
The number of SCD/SCA in football players did not increase during the COVID-19 pandemic when compared to an equivalent period before. Specifically, our data did not show an increase in cases during the COVID-19 pandemic as it would be expected from a higher number of SARS-CoV-2-related myocarditis or CAD. This may be even more significant when considering the raised awareness for CAD and myocarditis during the pandemic as well as the overall upward trend in recorded cases within the FIFA Sudden Death Registry over the years (learning curve) [5].
These numbers cannot explain reasons why there was no increase of SCD/SCA cases, regardless of whether they are due to myocarditis or CAD. One possible explanation is virus-related, i.e., the severity of the infection has not led to relevant additional cardiac damage in this target population [7]. Notably, of 8 athletes with SCA due to myocarditis between January 1, 2020, and June 30, 2022, none were attributed to COVID-19 [8]. Alternatively, management of the disease or its complications might have been improved quickly enough over the pandemic. Additionally, based on large concerns about COVID-19-related myocarditis potentially leading to myocardial injury in young athletes, [9] an extensive screening policy was initiated. This may have led to a relevant proportion of myocarditis cases that were identified and affected players temporarily disqualified from training and competition which may have saved them from SCD/SCA. However, this effect has probably been confined to professional or high-level sport and is, thus, not of major influence on these numbers. Compared to the general population, in which cardiac involvement due to COVID-19 was found in rates up to 4.2%, athletes were shown to have a much lower rate (0.5–2.4%) [10]. In addition, preventive measures such as physical distancing, lockdowns, travel bans and isolation of infected individuals may have limited transmission of SARS-CoV-2 and, thus, the development of myocarditis [11]. Nevertheless, SCD/SCA cases showed a slight upward trend in the summer months during the pandemic (pronounced in the second summer, 2021, Fig. 1), which may be related to fewer contact restrictions. It can be therefore speculated whether the partially enforced training break may have led to a higher risk of resuming football in football players with confirmed cardiovascular involvement due to COVID-19.
Limitations
It is important to consider the context and limitations of our findings, particularly given the unique circumstances created by the COVID-19 pandemic and the resulting global restrictions on sporting activities. Moreover, the most important limitation of our data is the lack of mandatory case reporting. Reliance on our online reporting platform and media search for data collection may have led to inaccuracies in determining diagnoses. Moreover, the global nature of the FIFA Sudden Death Registry means that data may be subject to different reporting standards and diagnostic criteria in different countries, further impeding interpretation of the results. This could be the reason why the exact cause of death remained unclear in a relevant proportion of cases.
Other reasons for underreporting might be that players took overproportionally long breaks from training after COVID-19 due to concerns about negative consequences or that they were monitored more closely compared to other infections before the pandemic. Moreover, it is possible that an SCD/SCA was not witnessed during individual training due to contact restrictions and therefore not reported in the media, whereas such an event would be very unlikely in an official match.
During the pandemic, especially at its peak, most sporting activities were suspended or severely restricted, with only elite football continuing in many countries. This means that the population studied during the lockdown consisted largely of elite football players, potentially skewing the comparison with a corresponding period before the pandemic, which included a wider range of football playing levels. The restriction to elite players during lockdown could have led to a selection bias, as these athletes typically undergo more rigorous medical screening and monitoring, which could have led to a different baseline risk profile for SCD/SCA. However, the proportion of elite players in our study population was low (< 10% in both periods, Fig. 1) and the potential bias was limited to the cumulative time of national lockdowns, which accounted for a maximum of 24% (9 out of 38 months) of the pandemic period (in most countries < 6 months, 16%) [12].
There was also a lower-than-optimal percentage of autopsy or medical reports due to availability, family interference, country–specific laws, cultural and religious reasons. Still these factors have not changed which makes a biasing influence unlikely. In addition, a lower proportion of myocarditis and CAD cases during the pandemic may to some extent be related to the lockdowns during which football training and matches were suspended. Although, as expected, only a few SCD/SCA were recorded in elite football, it must be taken into account that the potential exposure time was lower due to match cancellations and training interruptions during the COVID-19 pandemic, particularly in amateur football. Nevertheless, adjusting the event rate for the duration of exposure (cases per hour of training or match) was methodologically not possible due to the high variability in lockdown periods in various countries.
Taken together, it is crucial to consider that the data observed during the pandemic may be influenced by several factors, including changes in player health monitoring protocols, the return to high-performance sports after lockdowns and the potential impact of COVID-19 itself. To draw definitive conclusions, further studies are needed that specifically investigate the relationship between vaccination status (difficult to assess) and SCD/SCA in players. The pandemic also led to unprecedented disruptions to training and competition schedules, which could affect players' conditioning and cardiovascular health and potentially increase their susceptibility to SCD/SCA.

留言 (0)