
記住我






There were three males (75.0%) and one female (25.0%) included in our research. The mean age at surgery was 2.5 ± 0.5 years. Three patients (75.0%) had hyperopia, while one (25.0%) had myopia. All the patients presented with horizontal exotropia; the median degree was 55 (range = 40 to > 90) PD. Only one patient (25.0%) exhibited clinically significant limitations (−3 limitation on a scale of 0 to −4) [5] of ocular movements. Abnormal head position was observed in one patient (25.0%). Congenital hypoplasia of the MR muscles was revealed in all the patients during strabismus surgery, while one patient was also with hypoplasia of the LR muscle. We enhanced the surgery amount in three patients, and remained the surgery plan in one patient. Good correction of exotropia was achieved in all patients. Hypoplasia of the rectus muscles was not identified by postoperative MRI in three patients (75.0%). Main clinical data of the 4 cases were summarized in Table 1. All the cases are presented as follows.
Table 1 Main clinical data of 4 cases with congenital hypoplasiaCase 1Medical history and ocular findingsA 2-year-old girl presented with left exotropia that had begun at the age of 6 months. There was no family history of strabismus. The patient was healthy with no history of systemic disease. Cycloplegic refraction revealed a value of + 1.75 DS in the right eye and + 2.25 DS in the left eye. She had 60 PD of left exotropia, as determined by the prism alternating cover test (PACT) in the primary position (Fig. 1A). Ocular movement examination indicated a mild adduction limitation (−1 limitation on a scale of 0 to −4) in the right eye, along with overaction of the left inferior oblique (Fig. 1A). Fundus and ultrasound examinations showed no abnormalities. The patient was diagnosed with constant exotropia with left inferior oblique overaction (IOOA); she underwent corrective surgery in both eyes.
Fig. 1
Case 1: A 2-year-old girl with hypoplasia of the right MR and IR muscles. A Preoperative picture showing 60 PD of left exotropia in the primary position. B Surgeon’s view showing absence of the LR (left) and MR (right) muscles in the right eye. C Postoperative MRI scans showed bilateral orbital asymmetry and slight thinning of all EOMs. D Biopsy of the left MR muscle (left) revealed collagen and vascular tissue with scattered inflammation (left arrows) compared with normal muscle (right arrows). E At 1 month after surgery, the patient showed little horizontal deviation (< 5 PD) in the primary position but with right IO overaction
Preoperative surgical planForced duction test (FDT), left MR resection 5 mm, left LR recession 8 mm, right LR recession 8 mm, and left inferior oblique (LIO) anterior transposition.
Surgical proceduresFDT revealed mild restrictions of adduction and abduction in the right eye, and posterior adhesions were suspected. Intraoperative exploration revealed that the MR and LR muscles in the right eye could not be reached with strabismus forceps (Fig. 1B). Dystrophy of the MR muscle was observed in the left eye. In order to correct the horizontal strabismus, we increased the surgical quantity of the horizontal muscles in the left eye. The surgical plan was modified as follows: left MR muscle resection 8 mm, left LR recession 9 mm, and LIO anterior transposition.
Outcome and follow-upPostoperative MRI scans showed bilateral orbital asymmetry and slight thinning of all EOMs. However, all EOMs were present, including the right MR and LR muscles (Fig. 1C). Biopsy of the left MR muscle revealed collagen and vascular tissue with scattered inflammation (Fig. 1D), indicating degeneration of the left MR muscle. The postoperative diagnosis was modified to non-concomitant exotropia, left IOOA, left MR muscle degeneration, and right EOM displacement.
Postoperative follow-upAt 1 month after surgery, the patient was orthophoric in primary gaze and with right IO overaction. (Fig. 1E).
Case 2Medical history and ocular findingsA 3-year-old boy presented with right exotropia that had been present since birth. There was a history of forceps use at birth. Cycloplegic refraction revealed a value of + 1.75 DS in the right eye and + 1.50 DS in the left eye. He had 50 PD right exotropia, as determined by PACT in the primary position (Fig. 2A). Ocular movement examination indicated a mild adduction limitation (−1 limitation on a scale of 0 to −4) in both eyes, along with overaction of the bilateral inferior obliques (Fig. 2A). Fundus and ultrasound examinations showed no abnormalities. The patient was diagnosed with intermittent exotropia (IXT) with bilateral IOOA; he underwent corrective surgery in both eyes.
Fig. 2
Case 2: A 3-year-old boy with hypoplasia of the left MR muscle. A Preoperative picture showing 50 PD of right exotropia in the primary position. B Surgeon’s view showing dystrophy of the MR muscle (arrow), which resembled connective tissue, in the left eye. C Postoperative MRI scans did not show any obvious abnormalities. D During 1 year of follow-up, the patient showed 5 PD right exotropia in the primary position
Preoperative surgical planFDT, left MR resection 5 mm, left LR recession 8 mm, and bilateral inferior oblique tenotomy.
Surgical proceduresIntraoperative exploration revealed dystrophy of the MR muscle, which resembled connective tissue, in the left eye (Fig. 2B). Furthermore, the left MR muscle was closely adhered to the Tenon's capsule. Although dystrophy of the MR muscle might reduce its force generation, its adhesion to surrounding tissues could potentially enhance the force exerted. Therefore, ultimately, we did not alter the surgical plan. The surgical plan remained as planned: left MR resection 5 mm, left LR recession 8 mm, and bilateral inferior oblique tenotomy.
Outcome and follow-upPostoperative MRI scans did not show any obvious abnormalities (Fig. 2C). However, biopsy of the left MR muscle revealed collagen and vascular tissue with scattered inflammation, indicating degeneration of the left MR muscle.
Postoperative follow-upAt 1 month after surgery, the patient showed no heterotropia in the primary position, and his ocular movement was normal. During 1 year of follow-up, the patient showed 5 PD right exotropia in the primary position. His ocular alignment remained stable (Fig. 2D).
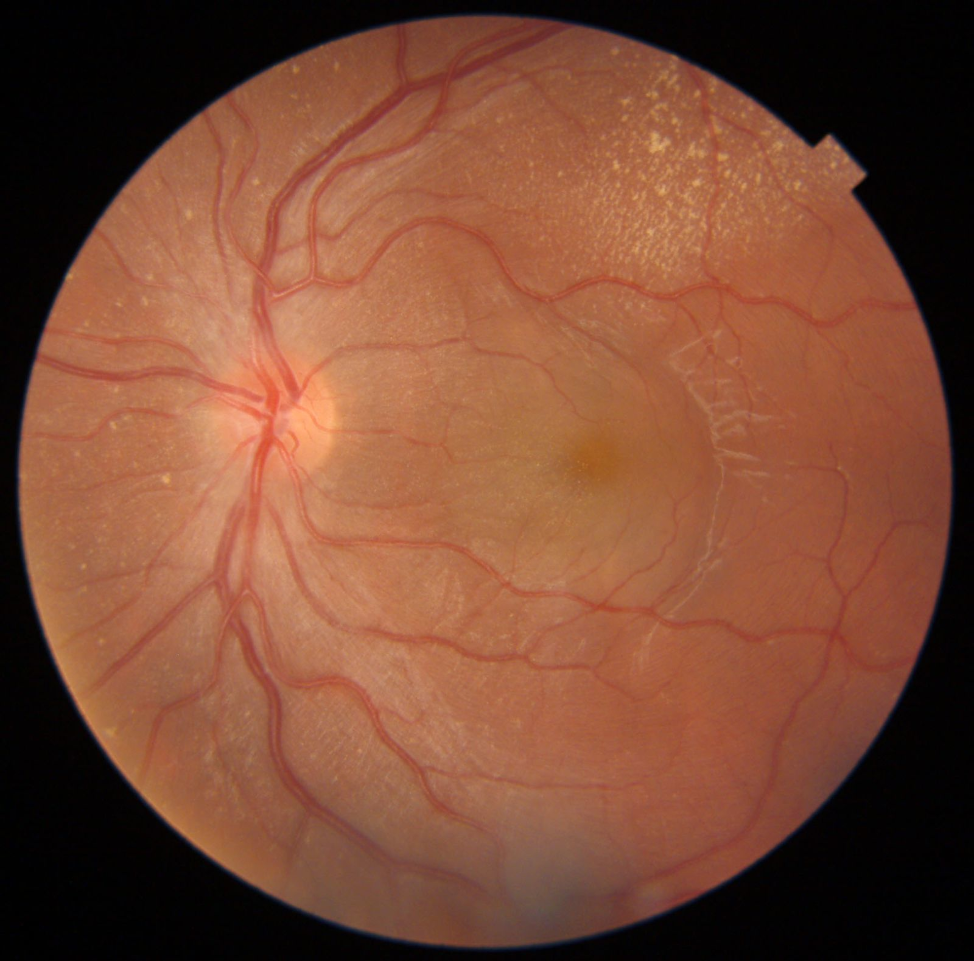
Case 3Medical history and ocular findingsA 3-year-old boy presented with left exotropia, which had been present since the age of 3 months. There was no family history of strabismus. Cycloplegic refraction revealed a value of + 0.00 DS in the right eye and −0.25 DS in the left eye. He had a large-angle exotropia (> 90 PD), as determined by PACT in the primary position (Fig. 3A). In both eyes, ocular movement examination revealed deficits of adduction beyond the midline (−3 limitation on a scale of 0 to −4) during elevation. Fundus photography revealed large cups in both eyes (Fig. 3B), while intraocular pressure monitoring and glaucoma screening did not reveal any abnormalities. Ultrasound examinations showed no abnormalities. The patient was diagnosed with constant exotropia, left IOOA and a physiological large cup-to-disc ratio; he underwent corrective surgery in both eyes.
Fig. 3
Case 3: A 3-year-old boy with hypoplasia of MR muscles in both eyes. A Preoperative picture showing a large-angle (> 90 PD) of left exotropia in the primary position. Three gaze pictures revealed deficits of adduction beyond the midline (−3 limitation on a scale of 0 to −4) during elevation in both eyes. B Fundus photography revealed large cups in both eyes. C Muscle fibers of the left MR muscle (left arrow) were thin. Surgeon’s view showing degeneration of the MR muscle (right arrow), which resembled connective tissue, in the right eye. D Postoperative MRI scans did not show any obvious abnormalities of the orbits or EOMs. E Good correction of exotropia was confirmed at the 2‑year follow‑up
Preoperative surgical planFDT, bilateral MR resection 7 mm, bilateral LR recession 9 mm, LIO anterior transposition.
Surgical proceduresDuring surgery, abnormal development of the MR muscles was observed in both eyes. The bilateral MR muscles resembled connective tissue and the muscle fibers were thin (Fig. 3C). Notably, normal muscle fibers were present 1 cm posterior to the bilateral MR muscles. Considering the partial dystrophy of the bilateral MR muscles, which might lead to a decrease in muscle elasticity, the surgical quantity was increased. The surgical plan was modified as follows: bilateral MR resection 9 mm, bilateral LR recession 9 mm, LIO anterior transposition.
Outcome and follow-upPostoperative MRI scans did not show any obvious abnormalities of the orbits or EOMs (Fig. 3D). Biopsy of the bilateral MR muscles revealed collagen fibers and vascular adipose tissue with scattered inflammation, indicating degeneration of the bilateral MR muscles.
Postoperative follow-upAt 1 month after surgery, the patient showed no horizontal deviation in the primary position and no underaction in any direction of gaze. Good correction of exotropia was confirmed at the 2‑year follow‑up (Fig. 3E).
Case 4Medical history and ocular findingsA 2-year-old boy presented with right exotropia (Fig. 4A) and a clinically significant left face turn (Fig. 4B). There was no family history of strabismus. The patient was healthy with no history of systemic disease. Cycloplegic refraction revealed a value of + 1.25 DS in the right eye and + 2.25 DS in the left eye. He had 40 PD right exotropia and 5 PD right hypertropia as determined by PACT in the primary position. Fundus and ultrasound examinations showed no abnormalities. Ocular movement examination indicated that the right eye did not elevate in adduction, and overaction of the right superior oblique muscle was observed. The patient was diagnosed with constant exotropia, along with superior oblique overaction (SOOA) and Brown syndrome in the right eye; he underwent corrective surgery in both eyes.
Fig. 4
Case 4: A 2-year-old boy with hypoplasia of the right MR muscle. A Preoperative picture showing 40 PD of right exotropia and 5 PD right hypertropia in the primary position. B The patient presented with a clinically significant left face turn. C, D Surgeon’s view showing absence of MR muscle (C), while other EOMs, such as the SO muscle (D), were thin in the right eye. E Postoperative MRI scans revealed the absence of the right MR muscle(arrow). F At 8 months after surgery, the patient demonstrated orthophoria in the primary position, along with vertical alignment abnormalities in upgaze
Preoperative surgical planFDT, right MR resection 5 mm, right LR recession 6.5 mm, and right superior oblique tenotomy on the nasal side.
Surgical proceduresFDT revealed a mild restriction of gaze toward the superior-medial position in the right eye. Intraoperative exploration revealed that the MR muscle in the right eye could not be reached with surgical forceps (Fig. 4C), while other EOMs were thin (Fig. 4D). Because of these intraoperative findings, the surgical plan was modified as follows: left LR recession 7 mm, right LR recession 6.5 mm, and right superior oblique tenotomy.
Outcome and follow-upPostoperative MRI scans revealed the absence of the right MR muscle (Fig. 4E).
Postoperative follow-upEight months post-surgery, the patient exhibited orthophoria in the primary position, along with vertical alignment irregularities during upward gaze. (Fig. 4F).
留言 (0)